Carcinomul de vestibul nazal – comentarii pe baza unui caz clinic
Carcinoma of the nasal vestibule – comments on a clinical case
Abstract
With an incidence of less than 1% of all head and neck neoplasia, basal cell carcinoma located in the nasal vestibule is a rare pathology in daily ENT practice, characterized by a nonspecific symptomatology. Surgery and radiotherapy are currently the most commonly used means to address it, however there is no generally agreed gold standard. The challenge that is posed then lies in performing a full surgical resection of the tumor mass while, at the same time, obtaining an aesthetically and functionally suitable outcome. The authors of this paper give an account of the clinical and therapeutic management particularities involved in the case of a 52-year-old patient with basal-cell carcinoma in the right nasal vestibule.Keywords
nasal vestibular carcinomasurgical treatmentRezumat
Întâlnit la mai puţin de 1% din totalitatea neoplasmelor capului şi gâtului, carcinomul cu localizare la nivelul vestibulului nazal este o patologie rară în practica ORL, cu un tablou clinic nespecific. Mijloacele terapeutice cel mai frecvent utilizate sunt chirurgia şi radioterapia, însă nu există un consens în ceea ce priveşte tratamentul de elecţie. Provocarea în această patologie este reprezentată de reuşita unei rezecţii tumorale complete cu limite de siguranţă şi cu obţinerea în acelaşi timp a unui rezultat estetic şi funcţional convenabil. Autorii prezintă particularităţile clinice şi managementul terapeutic în cazul unui pacient în vârstă de 52 de ani cu carcinom bazocelular de vestibul nazal drept.Cuvinte Cheie
carcinom vestibul nazaltratament chirurgicalIntroduction
Malignant tumors of the nose and paranasal sinuses account for 3% of the head and neck neoplasia. They occur more commonly in men, with a male-to-female ratio of 3:2, irrespective of location or histological types involved(1). Among these pathologies, less than 1% are nasal vestibule malignant tumors(2). Due to the anatomical features of the nasal vestibule, it could be argued that nasal vestibule tumors constitute a particular kind of pathology. Cone-shaped, with a maximum diameter of 1.5-2 cm, the nasal vestibule space lies between the nose wings, laterally, and the nasal septum, medially, being separated from the nasal cavity by limen nasi. Limen nasi serves as the junction between skin and the mucosa. It is lined with skin and contains sebaceous glands, sweat glands and hair follicles.
Among nasal vestibule tumors, well differentiated squamous cell carcinoma and moderately differentiated squamous cell carcinoma are the most frequently occurring histological types, with other commonly observed types being basal cell carcinoma and melanoma(2,3). Nasal vestibule neoplasia could be likened to skin neoplasia, progressing differently and having a better outlook than those of the nasal cavity or paranasal sinuses(2).
From a clinical standpoint, the main symptoms of most tumors occurring in the nasal cavity, sinuses and the nasal vestibule are unilateral obstruction, unilateral recurrent nosebleeds or, in the case of nasal vestibule tumors, an asymmetrically shaped nasal pyramid and localized swelling. About 6% of all cases also exhibit metastatic adenopathy. These, when present, constitute a negatively impacting factor on the overall patient prognosis(3).
A CT scan allows for a full assessment of the entire tumor mass, as well as evaluating the extent to which it may affect neighbouring structures. This, in turn, can be followed by an MRI scan in order to highlight the degree the tumor has spread to the nearby soft tissues.
The available treatment options include surgical resection, radiotherapy and chemotherapy. Surgery is often followed by undesirable aesthetic outcomes, which is why some authors recommend radiotherapy as a first course of action, with surgery only considered upon the failure of the former(1). At the same time, studies find similar results achieved through surgery, which has the added benefit of providing greater local control. Follow-up reconstructive procedures could mitigate some of the potential downsides(3,4).
According to the American Joint Committee on Cancer (AJCC), nasal vestibule tumors can be classified in four stages: T1 – primary tumors with a maximum diameter of 2 cm, T2 – tumors larger than 2 cm, but not exceeding 5 cm at their maximum diameter, T3 – tumors with a maximum diameter greater than 5 cm, and T4 – tumors extending to cartilages, bone or nerve structures(1). After reviewing this classification, Wang divided malignant nasal vestibule tumors into three stages, as follows: T1 – lesions limited to the nasal vestibule, relatively superficial, T2 – lesions extended to adjacent structures such as the nasal septum, upper lip, outer layer of the nasal pyramid and/or the nasolabial fold, without extending to the underlying bone, and T3 – lesions extending up to the hard palate, nasal turbinates and/or paranasal sinuses, extending to nearby muscle and bone structures(4).
Case report
The authors of this paper give an account of a clinical case of a 52-year-old patient, with no significant personal pathological history, who showed up at our clinic exhibiting a tumor mass located in the right nasal vestibule, accusing chronic obstruction and recurrent anterior nosebleeds in the right nostril, symptoms he had experienced for about a year prior.
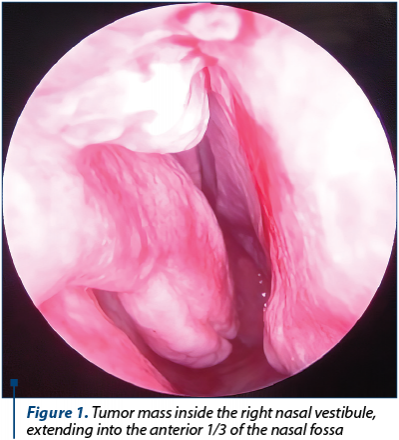
The ENT clinical examination and nasal endoscopy that have been performed revealed asymmetrical nostrils (right larger than the left one), swelling on the right side of the nasal pyramid, tensed dorsum nasi and right nasal wing caused by the presence of a protruding, sore tumor mass, bleeding upon examinations and occupying the lateral and upper part of the right nasal vestibule and the anterior part of the right nasal fossa (Figure 1).
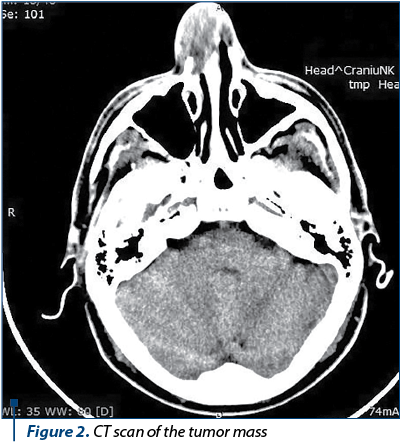
A CT scan revealed a nodular tumor mass developing in the right nasal vestibule, 22/32 mm wide and 19 mm long, irregular in shape and tissue density, with partial bone lysis in the right nasal bone and septum and moderate deformity of the right nasal wing (Figure 2).
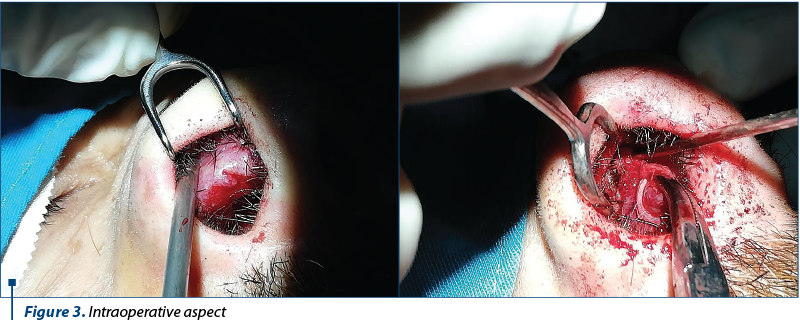
Considering all available clinical and paraclinical data, surgery was chosen as the preferred course of action, with the aim of performing a resection and a biopsy of the tumor mass. With the patient undergoing general anaesthesia and orotracheal intubation, an arched incision was made on the lateral wall of the right nasal vestibule. The process of detaching the tumor was hindered by the tumor mass extending towards the lateral pole of the right alar cartilage and the right triangular cartilage, coming into contact with the septal mucosa and the underlying cartilage from the anterior 1/3 of the anterior half of the nasal septum (Figure 3).
A one-piece resection was performed, removing the tumoral mass, together with the alar cartilage, triangular cartilage, mucosa and septal cartilage. The mass appeared to have a hard, fibrous consistency in the lateral half, while being soft, bleeding, with areas of necrosis in its medial part. At a macroscopic level, the right nasal bone was established to be the upper extent of the tumor, while the right middle nasal turbinate constituted the posterior boundary. Biopsy samples were collected from the upper, medial and lateral tumoral poles, for maximal safety margins. A fragment of the quadrilateral cartilage was used in place of the triangular cartilage, on the inner, upper side of the nasal dorsum, and secured by transfixing wire. The excised mass was sent to the pathological anatomy laboratory, pending histopathological diagnosis. According to Wang’s classification, the mass corresponds to stage T2 (Figure 4).

The histopathological diagnosis, as confirmed by performing immunohistochemical tests, was established to be moderately differentiated basal cell carcinoma, G2. The biopsy samples collected from the septal cartilage and mucosa of the upper half of the anterior 1/3 of the nasal septum, as well as the samples collected from the upper and lateral tumor poles as maximal safety margins showed a typical histological appearance.
Following these steps, the patient was referred to a specialized oncological committee. The committee then advised performing an MRI scan to provide a better overall post-surgery assessment without causing bud lesions, with increased contrast uptake in the mucosa and the right infraorbital nerve, as these constitute common post-therapeutic inflammatory changes. The patient was then discharged without pursuing further specialized oncological treatment.
Subsequent follow-up post-surgery check-ups did not find so far macroscopic signs of any potential leftover tumor residue. Aesthetically, the outcome of the intervention is satisfactory, in spite of the patient developing a small clogging area on the right nasal wing. Functionally, the outcome could be said to be a suitable one, as the patient managed to retain functionality of the right nostril respiratory pathways (Figure 5).

Discussion
Accounting for less than 1% of all head and neck tumors, malignant nasal vestibule tumors constitute a rare pathology. Nasal vestibule neoplasia mostly occurs in men, who make up around 55-70% of all cases, with an average age between 60 to 70 years old(2). Malignant nasal vestibule tumors include the following: squamous epidermal carcinoma, this being the most common histological type, basal cell epidermal carcinoma, undifferentiated carcinoma, glandular carcinoma, sarcomas, melanomas, and salivary malignancies (cylindroma)(1). As mentioned in the literature, prolonged sun exposure and smoking constitute increased nasal vestibular neoplasia risk factors. However, the precise nature of the relation between these factors and nasal vestibular cancer is not fully understood, literature data being insufficient due to a limited number of reported cases(2).
The symptomatology characteristic of the early stages of these tumors is nonspecific, being broadly defined by unilateral nasal obstruction, with the tumors extending to neighbouring structures as they progress, causing nosebleeds and/or facial deformities. Several studies cite the presence of metastatic adenopathy at the time of diagnosis and the localization of the tumor in the nasal septum as factors with a negative impact over the outlook, both in terms of patient survival, as well as of potential tumor regrowth(3,4). The existing nasal vestibular tumor classifications, as described in the literature, are not universally agreed upon and, so far, their accuracy has not been definitively proven. Moreover, there’s a diversity of views in regards to dealing with early stage tumors. Some authors recommend radiotherapy for likely yielding better outcomes, aesthetically, while others advocate pursuing a surgical intervention regardless of the tumor’s stage to ensure greater safety, whether or not pursued in conjunction with subsequent radiotherapy(1,4,5). There is, therefore, no standardized course of action for addressing these vestibular malignancies and a certain degree of controversy remains, both because of the rarity of these tumors, as well as due to their histological diversity, hard to reach location and extent.
In the case study detailed in this account, the authors opted for the surgical removal of the tumor mass and have done so using a mixed endonasal and endoscopic approach, allowing for greater surgical control. An element worthy of consideration is that multiple biopsy samples were collected during the intervention from the upper, medial and lateral poles of the tumor mass, in order to more accurately establish follow-up steps. Working within the anatomical constraints of the narrow nasal vestibule space, a one-piece resection was carried out, successfully removing the entire macroscopic area encompassed by the tumor mass. All biopsy samples collected turned out to be negative. In cases such as the one detailed in this paper, successful one-piece resections of the tumor mass, together with negative tumor safety margins biopsy results are decisive factors in the patient’s medium- and long-term prognosis.
After the histopathological diagnosis was confirmed through immunohistochemical examination, the patient was referred to a specialist oncological committee. After surgery, an MRI examination was carried out, the result of which did not reveal the presence of any potential leftover tumor residue. It was subsequently decided not to pursue any specific oncological treatment in this case, while continuing to actively monitor the patient.
Aesthetic and functional considerations regarding nasal vestibular surgery pose an added layer of difficulty. Since the tumor mass extended to the alar and triangular cartilages, a one-piece resection of the tumor mass and the two cartilages was the preferred course of action pursued. In order to address negative aesthetic considerations arising as a result of the intervention, an autograft created from a fragment of the quadrilateral cartilage was used in place of the triangular cartilage on the inner, upper side of the nasal dorsum, being secured in place by transfixing wire. Aesthetically, the outcome of the procedure is suitable, the patient exhibiting only minimal clogging of the right nasal wing. Currently, there are differences of opinion between practitioners on how to approach aesthetic considerations. While some authors favor specialized oncological treatment, others advocate for the greater safety provided by the full tumor resections, with subsequent reconstructive interventions carried out at a later stage, in a different procedure.
With the tumor mass being located in the internal nasal valve and extending to the anterior half of the right nasal fossa, the alar and triangular cartilage, resection proved challenging. The postoperative healing process was tedious, with multiple flanges and granulation tissue being formed, while adhesions had to be periodically removed. However, the careful management of the healing process resulted in a suitable, functional outcome, as the patient regained functionality of the right nostril respiratory pathways.
Conclusions
Malignant nasal vestibule tumors constitute a particular, rare pathology, accounting for less than 1% of all head and neck tumors. The difficulty in reaching the location and the extent of the tumor can pose a challenge for ENT practitioners. One-piece tumor resection, as well as the resection margins biopsy samples testing negative are important and decisive factors for the patient’s prognosis, increasing the patient’s chances of medium- and long-term survival.
Conflict of interests: The authors declare no conflict of interests.
Bibliografie
- Daele JJ, Vander Poorten V, Rombaux P, Hamoir M. Cancer of the nasal vestibule, nasal cavity and paranasal sinuses. B-ENT. 2005; 1(1): 87-96.
- Dagan R, Amdur RJ, Dziegielewski PT. Cancer of the nasal vestibule, Feb 2019, available at www.uptodate.com.
- Taxy JB. Squamous Carcinoma of the Nasal Vestibule - An Analysis of Five Cases and Literature Review. American Journal of Clinical Pathology. 1997; 107 (6): 698-703.
- Horsmans JDJ, Godballe C, Jørgensen KE, Bastholt L, Løntoft E. Squamous cell carcinoma of the nasal vestibule. The Journal of Laryngology & Otology. 1999; 37: 117-121.
- Ledderose GJ, Reu S, Englhard AS, Krause E. Endonasal resection of early stage squamous cell carcinoma of the nasal vestibule. European Archives of Otorhinolaryngology. 2014; 271(5): 1051-1055.

The First National Congress of the young Romanian Society of Audiology and Communication Pathology
Sebastian Cozma
Between the 12th and 14th of September 2019, we had the joy of meeting in a special academic and cultural setting offered by the Palace of Culture in Iaşi, on the occasion of the First National Congre...
Aspecte particulare ale anatomiei etmoidale pe imagini CT
Alexandra Gheorghe, Silviu Crăc, A. Panfiloiu, Vlad Andrei Budu
Anatomia ilustrată pe descoperirile imagistice reprezintă baza înţelegerii structurilor normale şi patologice rinosinuzale. Actualmente, radiologia convenţională a fost înlocuită de imagistica CT, noul standard de au...
Utilizarea pivoturilor endodontice în restaurările odontale armate pe dinţi devitali
Irina-Maria Gheorghiu, Paula Perlea, Claudiu-Gabriel Ciolan, Loredana Mitran, Mihai Mitran, Alexandru Iliescu
În situaţiile clinice în care se impune restaurarea distrucţiilor coronare masive, este obligatorie utilizarea mijloacelor suplimentare de retenţie ce pot asigura succesul şi menţinerea restaur...
Frontal sinus osteoma – case report
Celesta Drăgulescu, M. Chițac, A. Weisman, M. Condrat, X. Dolghii, Emanuela Onisâi, M. Vasilca
Osteomul reprezintă o tumoră benignă a sinusurilor paranazale, afectând cu predilecţie sinusul frontal. Are o evoluţie lentă şi silenţioasă, fiind descoperit adesea accidental prin examenul CT efectuat pentru diagnosti...
Polipoză de sinus frontal operată prin abord endoscopic transcranian
Bogdan Mocanu, Silviu Oprescu
Prezentăm cazul unui pacient, în vârstă de 62 de ani, cu o formaţiune tumorală voluminoasă de sinus frontal bilateral, cu sindrom cefalalgic sever şi distrucţia parcelară a laminei papiracee stângi şi a peretelui posterior al sinusului frontal drept. Abordul endoscopic s-a efectuat printr-o fereastră interspr...