Rare clinical features in non-Hodgkin lymphomas of the head and neck
Semne clinice rare în limfomul non-Hodgkin de cap şi gât
Abstract
Lymphoma is the second most frequent malignant diagnosis of the head and neck, following squamous cell carcinoma. The most common form of manifestation of lymphomas in the ENT practice is cervical polyadenopathy. This paper presents two cases in which the clinical presentation was not typical for a head and neck lymphoma. The first case presents an ulceration of the tonsillar fossa and a laterocervical lymph node block, while the second case presents a parotid tumor. In both cases, the final diagnosis was non-Hodgkin lymphoma. Lymphoma should be taken into consideration when making the differential diagnosis of a tumor formation in the head and neck, regardless of its ulcerated or hypertrophic, exophytic or infiltrative form. For an accurate and prompt diagnosis, close collaboration between the otorhinolaryngologist and the pathologist is necessary.Keywords
lymphomatonsillar ulcerationparotid gland tumorRezumat
Limfomul este cel de-al doilea diagnostic malign, după carcinomul scuamos, cu localizare la nivelul capului şi gâtului. Cea mai frecventă formă de manifestare a limfoamelor din sfera ORL este cea de poliadenopatii cervicale. Această lucrare prezintă două cazuri la care prezentarea clinică nu era cea tipică pentru un limfom din sfera capului şi gâtului. Primul caz prezintă o ulceraţie la nivelul lojei amigdaliene şi un bloc adenopatic laterocervical, iar cel de-al doilea caz prezintă o formaţiune tumorală parotidiană. În ambele cazuri, diagnosticul final a fost de limfom non-Hodgkin. Limfomul trebuie luat în considerare atunci când se realizează diagnosticul diferenţial al unei formaţiuni tumorale de la nivelul capului şi gâtului, indiferent de forma sa ulcerată sau hipertrofică, exofitică sau infiltrativă. Pentru un diagnostic corect şi rapid, este nevoie de o strânsă colaboare între medicul otorinolaringolog şi medicul anatomopatolog.Cuvinte Cheie
limfomulceraţie amigdalătumoră parotidăLymphoma is the second most frequent malignant tumor of the head and neck, following squamous cell carcinoma.
Risk factors for non-Hodgkin lymphoma (NHL) include immunodeficiency, exposure to chemicals such as glycophosphate, a history of chemotherapy and radiation therapy, and infection with EBV. In the literature, infections with hepatitis C virus, Helicobacter pylori, human T-lymphotropic virus 1 or herpesvirus 8 are also cited as having an important role in the development of NHL(1). Usually, patients with NHL are over 60 years old, with an incidence that is 1.5 times higher in men than in women.
The two most frequent histopathological subtypes are diffuse large B-cell lymphomas and follicular lymphomas.
The clinical presentation of these lymphomas most commonly takes the form of laterocervical lymphadenopathy or may involve the lymphoid tissue of the Waldeyer’s ring. In the latter case, it appears as a tumor in the nasopharynx or may cause hypertrophy of a palatine tonsil. Unlike squamous cell carcinoma, lymphoma usually appears as a non-ulcerated tumor mass(2).
In addition to local signs and symptoms, depending on location, constitutional symptoms, known as B symptoms, may also occur in one-third of patients. These include a weight loss of more than 10% of the initial weight and a temperature higher than 38°C in the absence of infection, or night sweats.
Lymphoma with ulceration in the tonsillar fossa
We present the case of a 72-year-old male patient from the rural environment who presented to the ENT department with dysphagia and the appearance of a large right supraclavicular tumor mass with a progressive increase in size for approximately five months. As for his medical history, the patient is known to have essential hypertension, type 2 diabetes mellitus and dyslipidemia.
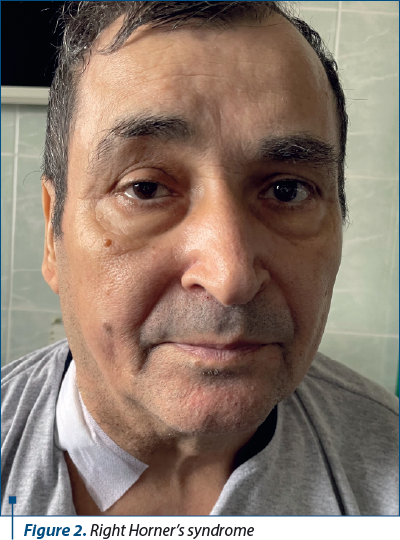
The ENT clinical examination revealed a bulky laterocervical and right supraclavicular lymph node mass, which was firm and fixed to deep planes, an ulcerated tumor in the right tonsillar fossa (Figure 1), and right Horner’s syndrome (Figure 2). On laboratory analysis, the patient presented an incomplete inflammatory syndrome, mild azotemic retention syndrome and hyposmolarity.

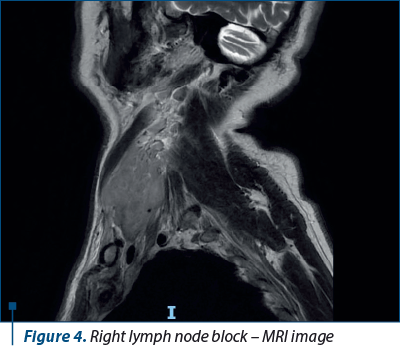
The cervical MRI examination revealed a tissue mass measuring up to 22/23 mm transaxial and 33 mm craniocaudally, with increased intermediate T2 signal, isointense T1 signal, diffusion restriction and contrast uptake, located at the level of the right palatine tonsil and possibly extending to the right soft palate (Figure 3). Additionally, a lymph node block measuring up to 56/47 mm transaxial and 72 mm craniocaudally was highlighted, involving groups III and IV on the right side. It displayed an intermediate T1/T2 signal, diffusion restriction, and no necrosis. The lymph node block compressed the right internal jugular vein, came in contact with the right common carotid artery on approximately half of its circumference, without clear signs of invasion or caliber modification, caused inflammatory signal changes at the level of the overlying soft tissues (including along the infrahyoid muscles on the right side) and extended medially to the right tracheoesophageal and paraesophageal grooves. Lymphadenopathy with similar characteristics was also described in the level II groups and supraclavicular region (Figure 4).

The suspicion of tonsillar carcinoma with lymph node metastases was raised, and a biopsy from the ulcerated right tonsillar tumor was performed under local anesthesia. The initial histopathological result was inconclusive, indicating chronic inflammatory infiltrate and necrotic areas in the examined specimen.
The patient returned to the clinic after one week for another biopsy. The initial symptomatology was accompanied by dyspnea (predominantly in dorsal decubitus) and dysphonia. Rhinopharyngolaryngoscopy revealed reduced mobility of the right vocal cord.
Under general anesthesia and orotracheal intubation, an incisional lymph node biopsy was performed at the level of the right supraclavicular lymph node block, as well as a biopsy at the level of the right palatine tonsil. The intraoperative histopathological examination of the lymph node block described a malignant proliferation consistent with lymphoma.
The periprocedural treatment consisted of the administration of cephalosporines, gastric antisecretory agents, antiemetics, and a small dose of hydrocortisone. The postoperative evolution of the right supraclavicular wound was favorable, with the removal of the surgical drain at 24 hours and suture removal at 10 days.
The dysphagic syndrome showed mild improvement during hospitalization, while dyspnea in dorsal decubitus partially improved with corticosteroids and an anti-Trendelenburg position.
Further imaging investigations were completed with a chest CT scan, which revealed multiple mediastinal lymphadenopathies and lymphadenopathy in the hepatic hilum.
The histopathological examination on paraffin-embedded tissue and immunohistochemical examination confirmed the diagnosis of non-Hodgkin lymphoma, both in the cervical lymph nodes and in the right palatine tonsil.
Secondary parotid lymphoma
A 68-year-old male patient from the urban area presented to the ENT department for the appearance of a left parotid tumor for approximately one month. He reported that the tumor appeared after a dental extraction performed in the left upper dental arch.
From the patient’s medical history, it was noted that he was diagnosed six years before with stage IV S, B follicular-type non-Hodgkin lymphoma. He underwent six cycles of R-CHOP chemotherapy between 2018 and 2019, followed by eight maintenance cycles with rituximab between 2019 and 2020. According to clinical, laboratory and imaging investigations performed every 3-6 months, the patient was in complete remission.
The clinical examination revealed a tumor of approximately 4/5 cm, poorly defined within the parotid tissue, firm in consistency and mobile. No other cervical lymphadenopathies were detected (Figure 5).

Before coming to the hospital, the patient underwent an orthopantomogram, which did not reveal any dental infectious foci.
Laboratory tests revealed dyslipidemia. Serology for hepatitis B, C and HIV was negative.
The patient underwent ultrasound-guided fine needle aspiration of the left parotid gland. The cytological examination revealed inflammatory tissue cells, establishing the diagnosis of chronic parotitis.
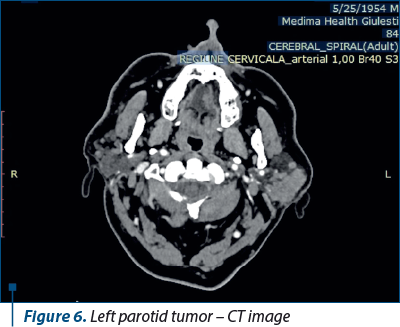
Given the patient’s history of hematological disease, a hematology consultation was performed, after which a reevaluation of imaging was decided. Contrast-enhanced computed tomography (CT) of the cervical, thoracic, abdominal and pelvic regions was performed. The only detected modification on the CT scan was located in the parotid gland, where a tumor formation measuring 41/19/49 mm was described in the left superficial parotid lobe. The lesion was associated with intraparotid lymphadenopathies (Figure 6).
Under general anesthesia, an arched incision was made in the left retromandibular skin fold, and the parotid gland was visualized. An infiltrative, indurated tumor formation was found, accompanied by multiple satellite lymphadenopathies measuring a maximum of 1/1 cm, with an elastic consistency. Excisional biopsy of a lymph node and incisional biopsy of the tumor formation were performed. The intraoperative histopathological examination established the diagnosis of lymphoma. The closure of the parotid gland capsule was performed using absorbable sutures, a drain was inserted, and an intradermal skin suture was applied. The drain was removed after two days, and the intradermal suture was removed after ten days.
The patient received perioperative treatment with Cefort®, gastric antisecretory agents, and low-dose corticosteroids.
The immunohistochemical examination confirmed the final diagnosis of large B-cell lymphoma.
Discussion
Most commonly, lymphoma involving the oral cavity presents as tonsillar hypertrophy. According to a study by Silva et al., other manifestations, in the order of frequency, include swelling, pain, paresthesia and abnormal tooth mobility. The first site of involvement in the oropharynx and oral cavity is the tonsils, followed by salivary glands, maxilla, mandible, palate and gums(3). The ulcerated appearance of the lesion in the presented case could be mistaken for ulcerated tonsillitis. The first sign was encountered in 50% of intraoral lymphomas, and the lesion can be confused with an infection(4,5).
The lymphadenopathy found in the case of the patient with ulceration in the tonsillar region mainly involves stations IV-V, which is atypical for tonsillar carcinoma, where lymph node metastasis generally occurs in stations II-IV, with rare occult metastases in stations I or V(6).
Salivary gland lymphomas present as painless tumor masses that progressively increase in size. They are most commonly mistaken for other tumor formations frequently encountered in salivary glands, such as pleomorphic adenoma or Warthin’s tumor. Radiologically, lymphoma of the parotid gland can be confused with lesions found in HIV patients or with Sjögren’s syndrome, as all of these pathologies can exhibit multiple solid nodules, cystic lesions or punctate calcifications(7). In the case of our patient, the imaging appearance was that of a dominant solitary nodule with multiple smaller satellite nodules.
Fine needle aspiration biopsy is the first-line approach for parotid tumor formations and can be used as a screening method for the diagnosis of head and neck lymphomas, with an accuracy of over 85%(8). In cases of uncertain results where clinical suspicion of malignancy is high, the gold standard remains excisional or incisional biopsy with histopathological and immunohistochemical examination. Both cases presented initially had a histopathological diagnosis suggesting chronic inflammation. However, in the first case, due to the clinical and imaging suspicion of a malignant tumor, further steps were taken after the initial uncertain histopathological diagnosis, including a second biopsy from the tonsillar region and an incisional biopsy of the lymph node block. In the second case, considering the patient’s history of lymphoma, after the fine needle aspiration biopsy, it was decided to continue the investigations with an incisional biopsy.
Conclusions
Lymphoma should be considered in the differential diagnosis of a tumor formation in the head and neck, regardless of its ulcerated or hypertrophic, exophytic or infiltrative nature. For an accurate and timely diagnosis, a close collaboration between the otolaryngologist and the anatomopathologist is necessary.
Conflict of interest: none declared
Financial support: none declared
This work is permanently accessible online free of charge and published under the CC-BY.

Bibliografie
-
Hartage P, Wang S, Bracci P. Non-Hodgkin Lymphoma. Cancer epidemiology and prevention. pp. 898-918, 2006.
-
Morton LM, Wang SS, Cozen W, et al. Etiologic heterogeneity among non-Hodgkin lymphoma subtypes. Blood. 2008;112(13):5150-5160. doi:10.1182/blood-2008-01-133587.
-
Silva TD, Ferreira CB, Leite GB, de Menezes Pontes JR, Antunes HS. Oral manifestations of lymphoma: a systematic review. Ecancermedicalscience. 2016;10:665. Published 2016 Aug 17. doi:10.3332/ecancer.2016.665.
-
Colmenero C, Gamallo C, Pintado V, Patron M, Sierra I, Valencia E. AIDS-related lymphoma of the oral cavity. Int J Oral Maxillofac Surg. 1991;20(1):2-6. doi:10.1016/s0901-5027(05)80684-8
-
Abdelwahed Hussein MR. Non-Hodgkin’s lymphoma of the oral cavity and maxillofacial region: a pathologist viewpoint. Expert Rev Hematol. 2018;11(9):737-748. doi:10.1080/17474086.2018.1506326.
-
Da Mosto MC, Zanetti F, Boscolo-Rizzo P. Pattern of lymph node metastases in squamous cell carcinoma of the tonsil: implication for selective neck dissection. Oral Oncol. 2009;45(3):212-217. doi:10.1016/j.oraloncology.2008.05.004.
-
Stewart A, Blenkinsopp P, Henry K. Bilateral parotid MALT lymphoma and Sjögren’s syndrome. Br J Oral Maxillofac Surg. 1994;32(Issue 5):318-322. https://doi.org/10.1016/0266-4356(94)90055-8.
-
Karimi-Yazdi A, Motiee-Langroudi M, Saedi B, et al. Diagnostic value of fine-needle aspiration in head and neck lymphoma: a cross-sectional study. Indian J Otolaryngol Head Neck Surg. 2014;66(Suppl 1):277-280. doi:10.1007/s12070-012-0484-y.

Laureaţii primei ediţii a Galei Elitelor Medicale în Otorinolaringologia Românească
Două evenimente de excepţie în domeniul otorinolaringologiei au avut loc, în data de 21 aprilie, la Cluj-Napoca. Este vorba despre Forumul „Progrese şi Excelenţă în Otorinolaringologie” şi Gala Elitelor Medicale în Otorinolaringologia Românească, ambele desfăşurate sub egida Societăţii Române de Foniatrie. ...
Full zirconia single tooth fixed prosthetic restorations obtained through CAD/CAM technology – technological and practical aspects (Part II)
Mihai David, Alexandra Dragomir, Radu Cătălin Costea, Viorel Ştefan Perieanu, Manuela Popescu, Mădălina Violeta Perieanu, Liliana Burlibaşa, Ileana Ionescu, Mihai Burlibaşa
Tehnologia CAD/CAM reprezintă o alternativă inovatoare în protetica dentară, ce asigură o calitate maximă pentru toate tipuri...
Technological aspects in the reconstruction of the dental abutment with post and core restoration using the indirect method: modern versus digital
Camelia Ionescu, Andreea-Elena Vrabie, Radu Cătălin Costea, Viorel Ştefan Perieanu, Manuela Popescu, Mădălina Violeta Perieanu, Liliana Burlibaşa, Ileana Ionescu, Mihai Burlibaşa
Pierderea unei cantităţi semnificative de ţesuturi dure dentare de la nivel coronar impune utilizarea unui dispozitiv coronor...
The evolution of maxillary sinus surgery: open approaches in the era of nasal endoscopy
Anca-Ionela Cîrstea, Maria Dana Gheorghiev, Miruna Bratiloveanu, Lorena Păun, Rareş Oancă, Remus Chirciu, Mihai Dumitru, Daniela Vrînceanu
În domeniul otolaringologiei, managementul chirurgical al afecţiunilor sinusului maxilar a evoluat semnificativ odată cu apariţia .../32 - Maxillomandibular skeletal repositioning and the upper airways.webp)
Repoziționarea scheletală maxilomandibulară și căile respiratorii superioare: rezultate funcționale în cazurile de chirurgie ortognatică
Remus Chirciu, Matei Dumitru, Bogdan Bănică, Mircea Laslău, Rareş Oancă, Lorena Păun, Ionuț Costin, Daniela Vrînceanu
Repoziționarea scheletală maxilomandibulară (MSR) modifică relațiile spațiale ale limbii, palatului moale și pereților faringieni ...