Reconstrucţia unui defect complex ce cuprinde multiple subunităţi nazale cu lambou insular după chirurgia oncologică a carcinomului bazocelular
Nasal reconstruction of multiple nasal subunits skin defect using an “island flap” after oncological surgery for basal cell carcinoma
Abstract
Approximately 85% of basal cell carcinomas occur on the face(1). In nasal region, the sites include lateral nose walls, dorsum nasi, alar region or nose tip. Reconstructing defects in this area becomes challenging when soft tissue defects following skin tumors excisions either have a significant size, or they include two or more nasal subunits. For these patients, radical surgery with complete excision of the tumor results in exposure of nasal cartilages, thus requiring reconstruction with local flaps aiming to restore function and pleasant aesthetics.Keywords
skin carcinomabasal cell carcinomanasal regionnasal reconstructionlocal flapsRezumat
Aproximativ 85% dintre carcinoamele bazocelulare apar la nivelul feţei(1). În regiunea nazală, zonele includ pereţii nazali, dorsum nasi, cartilajele alare şi vârful nasului. Reconstrucţia defectelor în aceste zone devine o provocare când defectele de părţi moi rezultate din excizia tumorilor au fie dimensiuni mari, fie cuprind două sau mai multe subunităţi nazale. În cazul acestor pacienţi, chirurgia radicală, cu excizia completă a tumorii, poate rezulta în expunere de cartilaj nazal, situaţie în care este absolut necesară reconstrucţia cu lambouri locale, urmărind păstrarea funcţionalităţii şi rezultate estetice satisfăcătoare.Cuvinte Cheie
carcinoame cutanatecarcinom bazocelularregiune nazalăreconstrucţie nazalălambouri localeIntroduction
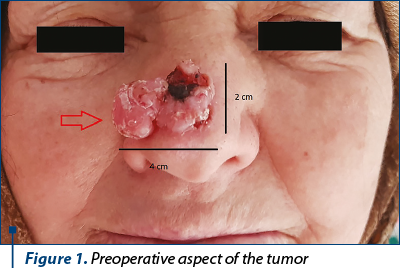
An 83-year-old female patient presents to our Department of Plastic and Reconstructive Surgery for a painless ulcerated tumoral mass, of approximating 4/2 cm, including nasal tip and the lower third of the dorsum nasi, in evolution for almost 7 years (Figure 1). She was under no current medication. She admits moderate sun exposure for the last 25 years. A thorough clinical exam revealed that the mass had a pedicle of approximately 1.5 cm in diameter located at the anatomical junction of the nasal tip, lateral walls and dorsum nasi, without reaching any of the nasal alas. The patient describes an initially slow evolution, from a small papule that kept on growing for about 5 years and a relative rapid progression in the last year. We performed a punch biopsy, confirming that the tumor was a basal cell carcinoma.
We decided to prepare the surgical treatment with the analysis of the future defect, considering its possible size and shape in the anatomical site and also the reconstruction options (Figure 2). After a thorough examination of patient’s general status, following interdisciplinary advice and patient’s refusal for local anesthesia, we decided to excise the tumor with 5 mm safety limits circumferentially, under general anesthesia.
Discussion
After excising the tumor with five millimeters safety margins, we had to consider the reconstruction of a 3/4 cm, oval defect which includes the tip of the nose, the inferior third of the dorsum nasi and the superior margins of both nasal lateral walls. The defect exposes the junction on the lower lateral cartilages and upper lateral cartilages (Figure 3), thus partial thickness and full thickness skin grafts were no longer an option for covering the defect.
The options for nasal reconstruction using locale flaps are either one-stage reconstruction or two-stage reconstruction. When it comes to large defects of the dorsum nasi, especially if the defect size exceeds 3 cm in diameter, forehead(2) flaps are, in generally, the preferred option. They have satisfying aesthetic result, the donor site can be closed either directly, in a “V-Y” manner, or covered with skin grafts. They are based on reliable vascular sources and usually have good rates of flap survival. The other two-stage(3) available flaps for these patients are nasolabial and check flap, zygomatic(4) island flap and axial fronto-nasal flap(5). The nasolabial and cheek skin flaps are excellent options for covering any part of the nose, used as unilateral or bilateral flaps, single flaps or combined with other local skin flaps, but the more the defect reaches the tip of the nose, usually the forehead skin flaps are being preferred.
The zygomatic flap is an axial pattern supplied by the zygomatic branch of the facial artery, which can provide good color match and satisfying scarring if the preoperative measurements are correct. It can cover defects up to 6/3 cm, but it is generally preferred for more vertical defects of the nose, along the dorsum nasi. We considered that we could not ensure tension-free sutures using this flap.
However, based on our patient’s anatomical characteristics, age and multiple other socioeconomical considerations such as the patient’s residence far from the hospital, with limited access to a health care provider, and the need to change wound dressings, we decided to cover the defect using a one-stage flap, the cheek island flap, based on the infraorbitary artery. The age associated laxity modifications and patient’s skin type allowed us to close the donor site per primam, hiding the scar in the naso-labial fold.
Results
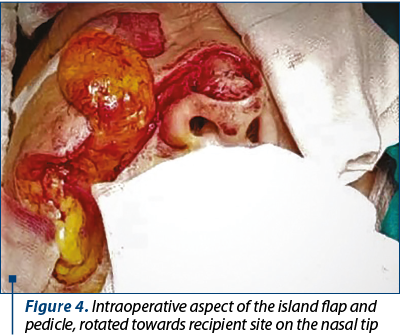
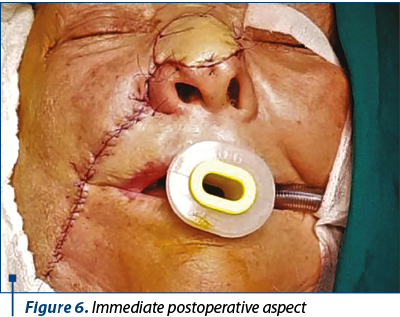
After excising the tumor, we made the incisions on preoperative markings and then elevated the flap, leaving a convenient pedicle width (approximately 2 cm) after careful measurements (Figure 4). After trimming the flap, we could close directly the donor site without considerable skin tension, hiding the scar in the nasolabial fold (Figure 5). The flap was sutured using horizontal mattress sutures with non-absorbable monofilament suture 6.0 (Figure 6).
Conclusions
The postoperative evolution was satisfying, with minimum ecchymosis or edema and moderate pain 6-8 hours after surgery (Figure 7). Seven days after surgery, the flap was fully integrated with acceptable color and texture match (Figure 8, Figure 9), with no complications. There was no need for any defatting procedures, but we noticed the pin-cushioning effect at the 6-week follow-up and decided to inject triamcinolone in the flap every three weeks in three sessions, with excellent cosmetic results (Figure 10). The final histopathological result revealed the complete excision of the tumor.






Conflict of interests: The authors declare no conflict of interests.
Bibliografie
- International Agency for Research on Cancer, 8090/3 BASAL CELL CARCINOMA, NOS. Available at http://codes.iarc.fr/code/4325. Accessed: August 21, 2018.
- Moolenburgh SE, McLennan L, Levendag PC, Munte K, Scholtemeijer M, Hofer SO, et al. Nasal reconstruction after malignant tumor resection: an algorithm for treatment. Plast Reconstr Surg. 2010 Jul.; 126(1):97-105.
- Strauch B, et al. Grabb’s Encyclopedia of Flaps. Wolters Kluwer, 2016.
- Masson JK, Mendelson BC. The banner flap. Am J Surg. 1977; 134:419.
- Gardetto A, Erdinger K, Papp C. The zygomatic flap: a further possibility in reconstructing soft tissue defects of the nose and upper lip. Plast Reconstr Surg. 2004; 113:485.

Rezolvarea endoscopică transnazală a unui condrosarcom rinosinuzal voluminos
Bogdan Mocanu, Silviu Oprescu, Anca Vișan
Condrosarcomul rinosinuzal este o tumoră malignă indoloră, agresivă la nivel local. Pacienţii se prezintă adesea pentru prezenţa unei tumori nedureroase, cu tulburări de vedere şi obstrucţie nazală. Aceste simptome sunt...
Reabilitarea chirurgicală a pacienţilor care au suportat intervenţia de evidare timpanomastoidiană totală
Sergiu Vetricean
Protejând pacientul de complicaţii, evidarea timpanomastoidiană totală (ETMT) nu asigură vindecarea sau încetarea procesului inflamator la nivelul urechii medii. Una dintre problemele actu...
Empiem subdural de origine otogenă – caz clinic
A. Sandul, M. Buracovschi, E. Eftodiev, N. Buracovschi
Empiemul subdural reprezintă o colecţie purulentă localizată între dura mater şi arahnoidă. Acesta apare, cel mai adesea, ca o complicaţie a unei infecţii rinosinuzale, a unei otite medii cronice supurate sau ca rezultat...
Consideraţii şi corelaţii statistice în cancerul de hipofaringe
Diana Maria Ciobîrcă, Elena Ioniță, Iulică Ioniță, Mircea-Sorin Ciolofan, Carmen-Aurelia Mogoanţă, Florin Anghelina, Ramona Denise Mălin, Alexandru- Nicolae Vlăescu, Eduard-Andrei Gheorghe, Manuela Guță, Irina Enache, Ioana-Cristina Oprişcan
Lucrarea prezintă un studiu statistic retrospectiv pe un lot de pacienţi cu neoplasm hipofaringian internaţi în Clinica ORL a Spit...
Particularităţile tratamentului chirurgical al pacienţilor cu melanoame faciale
Ioana Dumitrescu, Ştefania- Alexandra Stoica, Carina Chirilă
Melanomul cutanat este un cancer dezvoltat din melanocite, având ca principali factori de risc expunerea la radiaţii UV şi pielea deschisă la culoare. Melanomul reprezintă doar 1% din tumorile maligne cutanate, dar este ...