Tratamentul chirurgical al hemangioamelor cervico-faciale la copil – unde, când şi cum?
Surgical treatment for hemangiomas of face and neck in children – where, when and how?
Abstract
Introduction. Hemangiomas are among the most common benign tumors in children, with an incidence of 2-3% in newborns and up to 10% in the first year of life. The pathology at the level of head and neck accounts for 60% of the total number of cases with hemangiomas. In pediatric cases, most of them resolve spontaneously. Therefore, the therapeutic modalities should be applied in cases with an important esthetic deficit, with functional disturbances or with recurring bleeding. In children, the treatment should be preemptive in nature and requires the parents’ informed consent. Materials and method. We describe the case of a 9-year-old girl with hemangioma at the level of the right nasogenial groove. We applied our current algorithm for diagnosis and treatment and we performed the oral radical ablation of the hemangioma. Discussion. In pediatric cases, many of them have a spontaneous resolution. The indication for undergoing a treatment modality derives from major esthetic impact, functional disturbances or recurrent bleeding. Conclusions. The children with face and neck hemangiomas require a personalized approach tailored in a complex team meeting. Selective embolization should be performed in selected cases before surgical ablation by a trained interdisciplinary team.Keywords
hemangiomachildrensurgeryRezumat
Introducere. Hemangioamele sunt cele mai întâlnite tumori benigne ale copilului, având o incidenţă de 2-3% la nou-născut şi ajungând până la 10% în apropierea vârstei de 1 an. Localizarea la cap şi gât reprezintă 60% dintre toate cazurile de hemangioame. Indicaţia terapeutică în cazul hemangioamelor la copil trebuie să ţină cont de faptul că cele mai multe regresează spontan. Astfel, indicaţie terapeutică vor avea hemangioamele cu impact estetic semnificativ, cele care induc tulburări funcţionale sau cele cu sângerări recurente. Tratamentul hemangioamelor la copil este considerat preventiv şi necesită consimţământul informat al părinţilor. Materiale şi metodă. Prezentăm cazul clinic al unei fetiţe de 9 ani, cu un hemangiom al regiunii geniene drepte, la care s-a practicat ablaţie radicală prin abord oral. Prezentăm algoritmul de diagnostic şi tratament. Discuţie. Cele mai multe cazuri pediatrice au o rezoluţie spontană. Indicaţia de tratament se impune în cazul unui impact estetic semnificativ, al tulburărilor funcţionale şi al sângerărilor recurente. Concluzii. În hemangioamele cervico-faciale la copil, protocolul terapeutic trebuie individualizat. Discutarea acestui protocol trebuie făcută într-o echipă mixtă şi antrenată în această patologie. Embolizarea selectivă se poate face doar preoperatoriu, în cazuri selecţionate.Cuvinte Cheie
hemangiomcopilchirurgieIntroduction
Hemangiomas are some of the most common benign tumors in pediatric population, with an incidence of 3% at birth and reaching 10% till the age of 1 year old(1). Head and neck location represents 60% of the cases with hemangioma. There is a general female predominance(2). During their evolution, it is described a proliferative stage of up to 18 months followed by an involution stage with color change to wine-like red(3). Thus, 50% of the head and neck hemangiomas resolve by the age of 5, and up to 70% by the age of 7(4). Their etiology is still debatable. There is some association with older age of the parents, high blood pressure during pregnancy, and increased weight at birth(5).
Since 1982, Mulliken and Glowacki have classified vascular anomalies at birth in hemangiomas and vascular malformations(3). Hemangiomas represent, from a histological point of view, a proliferation of endothelial cells leading to formation of small vascular tumors with capillaries, venules and small vein. Given the type of vessels proliferating inside, the hemangiomas can be cavernous or capillary(1-3). Cutaneous hemangiomas may be superficial (inside papillary dermal layer), deep (inside reticular dermal layer or subcutaneous tissue) or mixt. This staging can be also applied to hemangiomas at the level of the mucosa. Furthermore, their clinical evolution undergoes three steps: proliferation in the first year, involution up to 5 years, and involuted up to 10 years(1,2,4).
The current principles of diagnosis in hemangiomas begin with thorough ENT clinical exam, searching for pulsations and murmurs implying the evolution of an arteriovenous malformation. Flexible endoscopy searches for associated oral and pharyngeal pathology. Doppler ultrasound is a noninvasive imaging modality for clinical monitoring. The gold standard is represented by cervical and cerebral MRI. Hemangiomas show a T1 hypo signal and T2 hyper signal along with contrast media uptake(5). Bilateral carotid angiography permits selective embolization before surgery in order to diminish bleeding. Hemangiomas without a surgical indication should not be embolized and benefit only from Doppler ultrasound and MRI follow-up. Selective embolization should be reserved only to those cases with active bleeding.
The differential diagnosis of hemangiomas focuses on solid tumors or other vascular tumors like lymphangiomas or arteriovenous malformations. The latter represent a direct connection between frail arteries and veins with the absence of capillaries and high-pressure blood passing between these two territories(4).
While facing such a case, the ENT surgeon should take into consideration the fact that many of the hemangiomas disappear spontaneously. The treatment modalities should be applied in those cases with increased esthetic impact, functional disturbances and recurrent bleeding. In children, the surgical removal is considered preemptive and requires parents’ or legal guardians’ informed consent(4).
Clinical case presentation
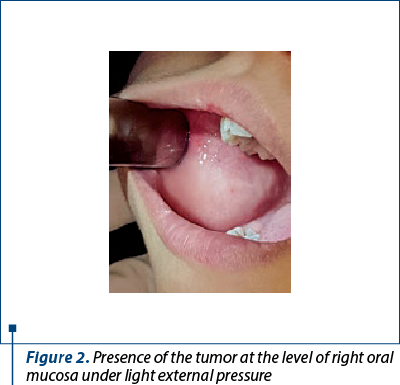
We encountered the case of a 9-year-old girl with a right genial tumor with debut two years before, painless but with increased dimensions during effort or mastication (Figure 1). The clinical exam revealed a soft mass, without pulsations and protruding through oral mucosa while pressing on the genial grove (Figure 2).


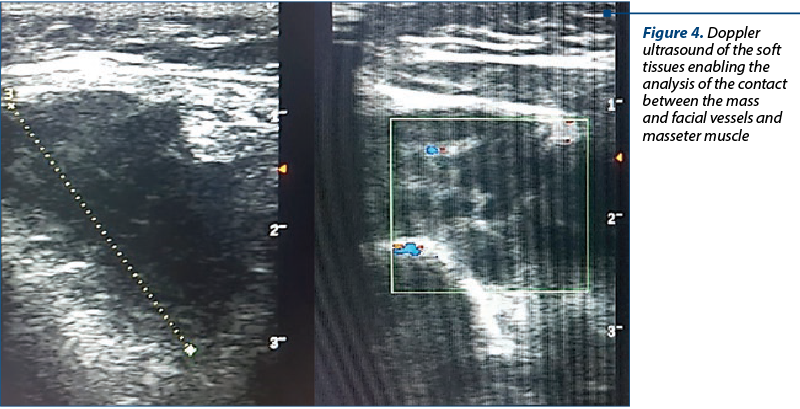
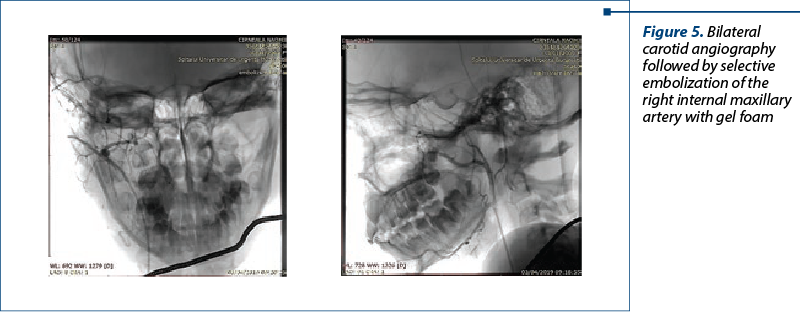
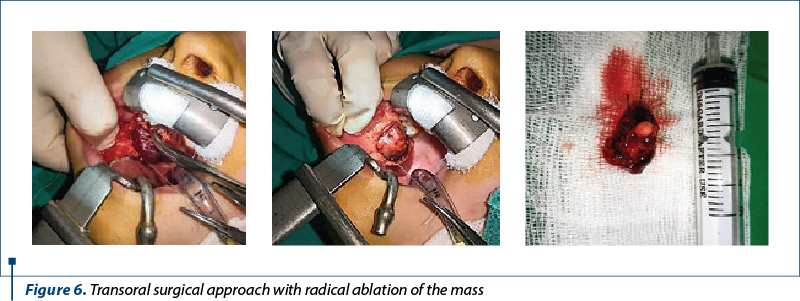
Cerebral MRI with contrast described a soft tissue mass in the right genial region with T1 hypo signal and T2 hyper signal (Figure 3). Doppler ultrasound both of facial soft tissues enabled further study of the relations between facial vessels and masseter muscle (Figure 4). Before surgery, we performed bilateral carotid angiography and selective embolization of the right internal maxillary artery with gel foam (Figure 5). Surgery was performed transoral under general anesthesia (Figure 6). Surgical healing was uneventful, with complete removal of sutures at 10 days (Figure 7). The pathology result concluded to a cavernous hemangioma.
Discussion
We still lack a clear recipe for approaching hemangiomas. Every case requires a personal and sequential therapy protocol. One of the most recent is the Treatment Guideline for Hemangiomas and Vascular Malformations of the Head and Neck (Head and Neck 2010)(4).
The available treatment principles range from watchful waiting to laser therapy, medicine therapy (topical steroids, betablockers), sclerotherapy, radiotherapy, or cryosurgery. Classic open surgery is not the first line of treatment(6-14).
Surgery is indicated in cases with hemangiomas at the tip of the nose and on the lips which are not responding to other treatment modalities, upper eye lid hemangiomas with visual impairment, esthetic impact of hemangiomas of the forehead and scalp, and in cases with recurrent bleeding episodes(4,8). Further desk reference should be sought in the Guidelines of Care for Hemangiomas of Infancy (American Academy of Dermatology)(15). Unfortunately, in cases affecting the oral or pharyngeal mucosa, the guidelines require further data.
The general practitioner should refer such cases to dermatologists, pediatricians, plastic surgeons, OMF surgeons, or ENT surgeons. Ideally, such cases should benefit from the input of an interdisciplinary team reuniting also imaging specialists and interventional radiologists. The experience gathered with each case improves the outcome of the next child with hemangioma of face and neck.

Conclusions
Regarding pediatric cases with hemangiomas at the level of face and neck, the therapy protocol should be custom tailored. All the steps should be approved by a complex team trained to approach such complex cases. Selective embolization should be performed only before surgery and in other instances postponed. All the necessary arguments to support surgical decision and close cooperation with the parents and their informed consent are necessary.
Conflicts of interests: The authors declare no conflict of interests.
Bibliografie
- Jacobs AH, Walton RG. The incidence of birthmarks in the neonate. Pediatrics. 1976; 58:218–222.
- Waner M, Suen JY. Management of congenital vascular lesions of the head and neck. Oncology. 1995; 9:989–994. 997.
- Finn MC, Glowacki J, Mulliken JB. Congenital vascular lesions: clinical application of a new classification. J Pediatr Surg. 1983; 18:894–900.
- Zheng JW, Zhou Q, Yang XJ, Wang YA, Fan XD, Zhou GY, Zhang ZY, Suen JY. Treatment guideline for hemangiomas and vascular malformations of the head and neck. Head Neck. 2010; 32:1088–1098.
- van Rijswijk CS, van der Linden E, van der Woude HJ, van Baalen JM, Bloem JL. Value of dynamic contrast-enhanced MR imaging in diagnosing and classifying peripheral vascular malformations. Am J Roentgenol. 2002; 178:1181–1187.
- Guidelines of care for cryosurgery. American Academy of Dermatology Committee on Guidelines of Care. J Am Acad Dermatol. 1994; 31:648–653.
- Al Buainian H, Verhaeghe E, Dierckxsens L, Naeyaert JM. Early treatment of hemangiomas with lasers. A review. Dermatology. 2003; 206:370–373.
- Frieden IJ, Haggstrom AN, Drolet BA, Mancini AJ, Friedlander SF, Boon L, Chamlin SL, Baselga E, Garzon MC, Nopper AJ, Siegel DH, Mathes EW, Goddard DS, Bischoff J, North PE, Esterly NB. Infantile hemangiomas: current knowledge, future directions. Proceedings of a research workshop on infantile hemangiomas, April 7-9, 2005, Bethesda, Maryland, USA. Pediatr Dermatol. 2005; 22:383–406.
- Chantharatanapiboon W. Intralesional corticosteroid therapy in hemangiomas: clinical outcome in 160 cases. J Med Assoc Thai. 2008; 91:S90–96.
- Greinwald JH Jr, Burke DK, Bonthius DJ, Bauman NM, Smith RJ. An update on the treatment of hemangiomas in children with interferon alfa-2a. Arch Otolaryngol Head Neck Surg. 1999; 125:21–27.
- Ho NT, Lansang P, Pope E. Topical imiquimod in the treatment of infantile hemangiomas: a retrospective study. J Am Acad Dermatol. 2007; 56:63–68.
- Léauté-Labrèze C, Dumas de la Roque E, Hubiche T, Boralevi F, Thambo JB, Taïeb A. Propranolol for severe hemangiomas of infancy. N Engl J Med. 2008; 358:2649–2651.
- Koay AC, Choo MM, Nathan AM, Omar A, Lim CT. Combined low-dose oral propranolol and oral prednisolone as first-line treatment in periocular infantile hemangiomas. J Ocul Pharmacol Ther. 2011; 27:309–311.
- Ogino I, Torikai K, Kobayasi S, Aida N, Hata M, Kigasawa H. Radiation therapy for life- or function-threatening infant hemangioma. Radiology. 2001; 218:834–839.
- Frieden IJ, Eichenfield LF, Esterly NB, Geronemus R, Mallory SB. Guidelines of care for hemangiomas of infancy. American Academy of Dermatology Guidelines/Outcomes Committee. J Am Acad Dermatol. 1997; 37:631–637.

Lista rezumatelor lucrărilor susţinute in cadul celei de-a XII-a ediţii a Forumului ORL.ro 2020
Lista rezumatelor lucrărilor susţinute in cadul celei de-a XII-a ediţii a Forumului ORL.ro 2020...
Artera etmoidală anterioară – implicaţii în chirurgia endoscopică endonazală
Vlad Andrei Budu, Silviu Crăc, Alexandra Gheorghe, I. Bulescu
Autorii îşi propun o trecere în revistă a anatomiei descriptive a arterei etmoidale anterioare, insistând atât asupra aspectelor imagistice şi endoscopice, cât şi a implicaţiilor acestora în chirurgia endoscopică endo...
Miringoplastia în perforaţiile cvasitotale ale membranei timpanice, cu spitalizare de 24 de ore
Vasile Ciuchi, Oana-Irina Popa
Autorii prezintă experienţa lor de peste doisprezece ani în reconstrucţia membranei timpanice cu perforaţii largi, cu spitalizare de 24 de ore. Este expusă schematic intervenţia chirurgicală, cu succesiunea timpil.../32 - Maxillomandibular skeletal repositioning and the upper airways.webp)
Repoziționarea scheletală maxilomandibulară și căile respiratorii superioare: rezultate funcționale în cazurile de chirurgie ortognatică
Remus Chirciu, Matei Dumitru, Bogdan Bănică, Mircea Laslău, Rareş Oancă, Lorena Păun, Ionuț Costin, Daniela Vrînceanu
Repoziționarea scheletală maxilomandibulară (MSR) modifică relațiile spațiale ale limbii, palatului moale și pereților faringieni ...
Septoplastia endoscopică – indicaţii, avantaje și dezavantaje
Bianca Buleandra, Simona Georgescu, Remus Chirciu, Rareș Oanca, Lorena Păun, Ionuț Costin, Miruna Bratiloveanu, Ioana Eftime, Mihai Dumitru, Daniela Vrînceanu
Septoplastia endoscopică este o tehnică modernă, minim invazivă, utilizată pentru corectarea deviațiilor septale, oferind o vizua...