Consequences of anemia in pregnancy upon the newborn – a cross-sectional study
Consecinţele anemiei în sarcină asupra nou-născutului – studiu transversal
Abstract
Background. Anemia in pregnant women is still an important public health problem. The consequences on the newborn, immediate or late, can range from mild to severe pathologies. Aims. The main objective of the study was to identify the correlations that might occur between iron deficiency anemia in pregnant women from Suceava county, Romania, and its consequences on the newborn. Materials and method. Data collection for the cross-sectional study was performed using a questionnaire given to pregnant women admitted to the “Sf. Ioan cel Nou” County Emergency Clinical Hospital, in Suceava, Romania, in 2017. The questionnaire completed by the interviewer provided both general data about the patients and data on gestational age, hemoglobin and hematocrit values, birth weight of the newborn, APGAR score and neonatal pathologies. Results. The prevalence of iron deficiency anemia in pregnant women was 48% (Hb<11.5 g/dl). No correlation was found between hemoglobin value and newborn weight (p=0.353), even though it ranged from 1360 g to 4510 g (mean weight = 3020 g), nor between the presence of anemia and gestational age (p=0.155), although there were 30% preterm and 70% term births. In contrast, anemia during pregnancy was associated with a lower APGAR score (p=0.024), with the occurrence of perinatal pathologies in the newborn, some of them of significant severity (p<0.0009), and with the occurrence of neonatal pathologies in 50% of newborns. Conclusions. This study has shown the major practical importance of prophylaxis of iron deficiency anemia in pregnant women, with a positive impact on conception product.Keywords
iron deficiency anemiaphysiological pregnancynewbornAPGARneonatal pathologiesRezumat
Date generale. Anemia la gravide este încă o problemă importantă de sănătate publică. Consecinţele asupra nou-născutului, imediate sau tardive, pot varia de la patologii uşoare la boli severe. Scop. Obiectivul principal al studiului a fost de a identifica corelaţiile care pot apărea între anemia feriprivă în sarcină la gravidele din judeţul Suceava şi consecinţele acesteia asupra nou-născutului. Materiale şi metodă. Colectarea datelor pentru studiul transversal s-a realizat prin intermediul unui chestionar administrat femeilor gravide internate la Spitalul Judeţean de Urgenţă „Sfântul Ioan cel Nou” din Suceava, România, în anul 2017. Chestionarul completat a furnizat atât date generale despre paciente, cât şi date privind vârsta gestaţională, valorile hemoglobinei şi hematocritului, greutatea la naştere a nou-născutului, scorul APGAR şi patologiile neonatale. Rezultate. Prevalenţa anemiei feriprive la gravide a fost de 48% (Hb<11,5 g/dl). Nu s-a constatat nicio corelaţie între valoarea hemoglobinei şi greutatea nou-născutului (p=0,353), deşi aceasta a variat între 1360 g şi 4510 g (greutate medie = 3020 g), şi nici între prezenţa anemiei şi vârsta gestaţională (p=0,155), deşi au existat 30% naşteri premature şi 70% naşteri la termen. În schimb, anemia din timpul sarcinii a fost asociată cu un scor APGAR mai mic (p=0,024), cu apariţia unor patologii perinatale la nou-născut, unele dintre ele de gravitate semnificativă (p<0,0009), şi cu apariţia unor patologii neonatale la 50% dintre nou-născuţi. Concluzii. Acest studiu a demonstrat importanţa practică majoră a profilaxiei anemiei feriprive la gravide, cu impact pozitiv asupra produsului de concepţie.Cuvinte Cheie
anemie feriprivăsarcină fiziologică nou-născutAPGARpatologii neonataleIntroduction
Iron deficiency anemia is a real public health problem for all ages. Its importance is given by the fact that it can occur in pregnancy, with consequences for the newborn and infant, but which can later be carried over to older ages.
It is well known that a variety of lifestyle factors can have negative effects on pregnancy, and some may be teratogenic(1). Maternal hemoglobin below 8 g/dl has been associated with a 2.7-fold increase in the risk of preterm birth and with a 3.1-fold increase in low birth weight due to increased prematurity and intrauterine growth retardation(2,3). Severe anemia is associated with an increased risk of motor and cognitive impairments, reduced amniotic fluid volume, fetal cerebral vasodilation and fetal death(2,4,5), and with death in approximately 30% of infants hospitalized with anemia without immediate blood transfusion(6). Perinatal mortality rates increase significantly when maternal Hb values are below 11 g/dL, increase 2-3-fold at values below 8 g/dL and 8-10-fold at values below 5 g/dL(7). Newborns of anemic and nonanemic mothers did not show significant differences in hematological values obtained from cord blood. However, at 3 months of age, serum ferritin levels were significantly higher in infants of non-anemic mothers, and also the anthropometric parameters were normal. Significantly decreased immune response, growth retardation, impaired tooth integrity and salivary gland dysfunction can occur in prenatally iron-deficient infants(6,8).
Iron supplementation during pregnancy positively influences APGAR score and fetal Hb level for three months after birth(7). Positive response to iron supplementation is when Hb>10.5 g/dl, ferritin is above 12 µg/ml or transferrin saturation is above 16%(10), but compliance with iron supplementation in pregnancy is generally low, with only 49.7% of pregnant women consistently taking supplements in the second and third trimesters of pregnancy(11). High doses of iron supplements, often up to 300 mg/day of ferrous iron, are usually prescribed for the treatment of iron deficiency anemia, but studies have shown that high doses may increase the risk of low gestational age weight of the fetus in the first and second trimesters(12).
One study has shown that depletion of iron stores without symptoms of anemia in early pregnancy poses a high risk of decreased fetal weight, even with moderate daily intake of iron supplements, and that optimal fetal birth weight is achieved when nonsmoking women enter pregnancy with BMI between 22 and 26 kg/m2, are not anemic, have iron store levels above 300 mg (reflected by serum ferritin levels above 30 µg/l) and receive moderate doses of prenatal iron supplementation during pregnancy, so that Hb values are maintained between 95 and 125 g/l(13).
The objective of the present research was to assess the consequences of anemia in pregnancy on the newborn, in order to draw conclusions with clinical applicability in practice.
Materials and method
This observational study was conducted on a group of pregnant women (N=54) admitted to the maternity ward of the “Sf. Ioan cel Nou” Emergency County Hospital in Suceava, Romania, between March and May 2017, a short but significant interval for the scientific approach. The study followed the principles outlined in the Declaration of Helsinki. After obtaining the agreement from the hospital scientific committee and the informed consent from the pregnant women, the interviewer completed a questionnaire in which general data from the Pregnant Women’s Notebook(14) were used, including some important for our study: gestational age, hemoglobin and hematocrit values, type of delivery, birth weight of the newborn, APGAR score, presence of neonatal pathologies and duration of hospitalization.
The database containing the pregnant women’s responses to the questionnaire was processed using specialized software (Microsoft Excel, Statistica 8.0, Medcalc 13.3.3, SPSS 18.0). The results were interpreted and processed graphically, after which the conclusions of the study were formulated.
Results
The age of mothers from our study ranged from 16 to 46 years old (mean age = 30). Gestational age ranged from 28 to 40 weeks, with a mean of 39 weeks. Of the total number of newborns, 26% were preterm (gestational age < 37 weeks).
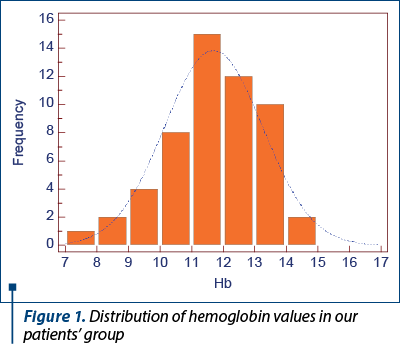
Regarding the assessment of anemia in pregnant women in the study group, hemoglobin values ranged from 7.7 to 14.5 g/dl (Figure 1). A percentage of 48% of the pregnant women had mild (Hb=9-11.5 g/dl) or moderate (Hb<9 g/dl) forms of anemia during pregnancy.
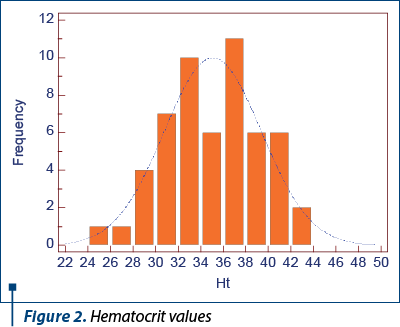
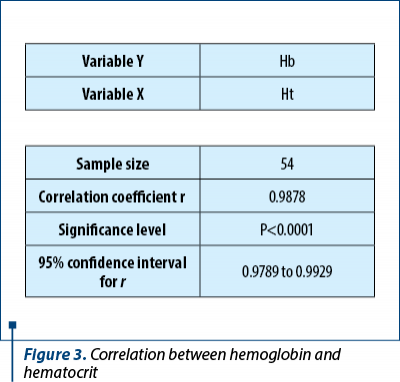
Hematocrit values ranged from 24% to 42% (Figure 2), which correlated statistically significantly with hemoglobin values (p<0.0001) – Figure 3.
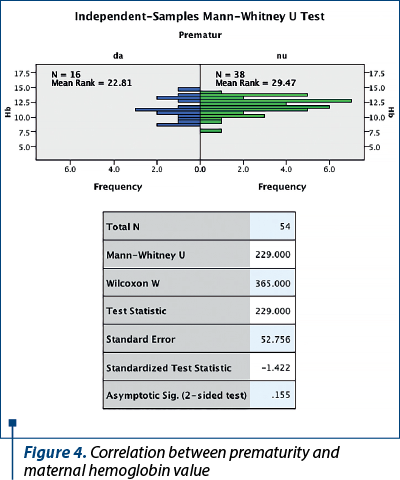
In the study group, there were 16 cases of premature births (30%) and 38 term births (70%). A correlation between hemoglobin value and gestational age was performed to see if there was a causal relationship. However, the nonparametric test did not test the hypothesis (p=0.155). Figure 4 shows that hemoglobin values are at approximately the same level in both groups.
Neither was newborn weight significantly influenced by maternal hemoglobin level (p=0.353), even though it varied between 1360 g and 4510 g (mean weight = 3020 g) – Figure 5.
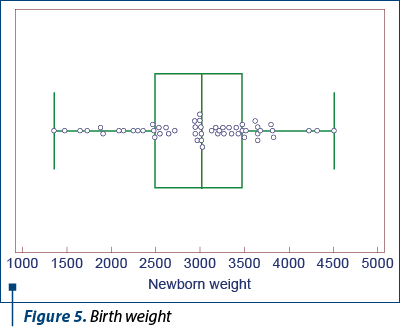
Although there are studies showing that the risk of preterm birth and lower birth weight are among the common consequences of iron deficiency anemia in pregnancy(7), the results of our study did not confirm this causal relationship.
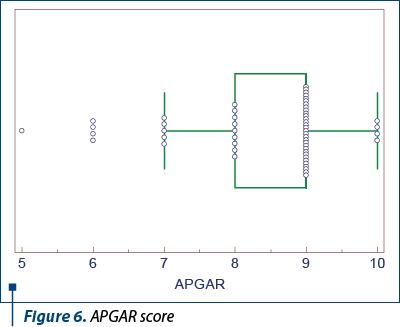
The APGAR score at birth ranged from 5 to 10 (mean APGAR = 9), indicating that generally the newborns had a favorable adaptation to extrauterine life and a good immediate prognosis (Figure 6).
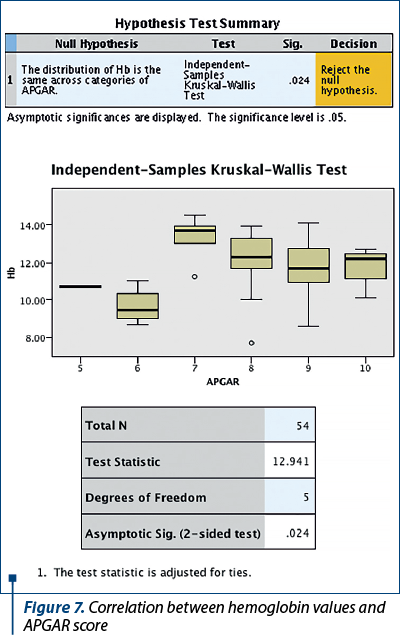
In contrast, in correlation with the hemoglobin values found in the patients in the study group, the lower APGAR score meant a more difficult neonatal adaptation to extrauterine life in the newborns of pregnant women with anemia (p=0.024) – Figure 7. Thus, there was a positive correlation between anemia in pregnancy and the lower APGAR score at birth.
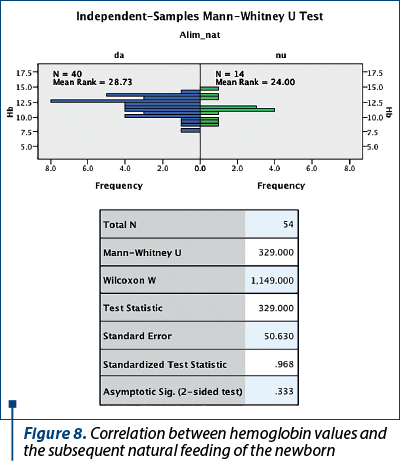
In our approach to study the influences of anemia in pregnant women on the infant, the statistical result showed that anemia during pregnancy did not influence the mother’s ability to breastfeed (p=0.333) – Figure 8.
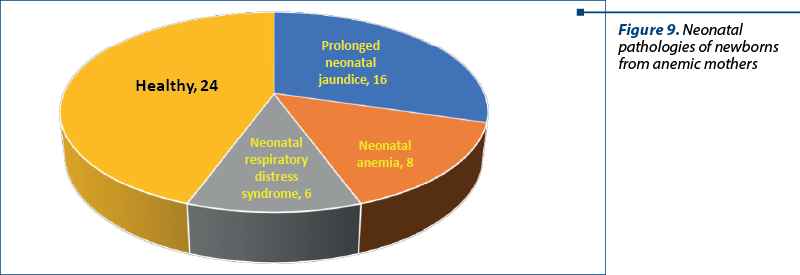
Regarding the occurrence of various pathological conditions in the neonatal period, these were most frequently represented by prolonged neonatal jaundice (26%; N=16), neonatal anemia (15%; N=8) and neonatal respiratory distress syndrome (11%; N=6). Also, 56% of the neonates (N=24) had no particular neonatal pathology (Figure 9).
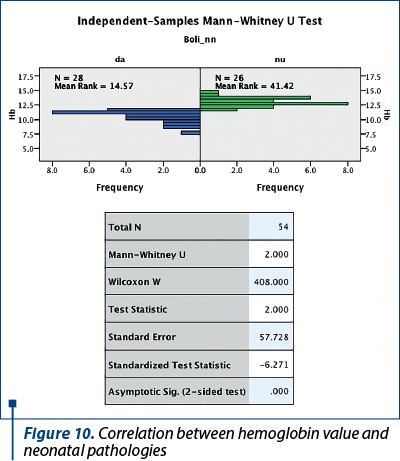
The statistical correlation between maternal hemoglobin value and the occurrence of perinatal pathologies in the newborn, some of them of significant severity, was significant (p<0.0009) – Figure 10, but anemia during pregnancy was a risk factor for the occurrence of neonatal pathologies in 56% of newborns (N=30).
Studies have shown that iron supplementation during pregnancy improves average fetal weight (by 6.46 g/month, along with folic acid)(9). The results of our study confirm these data (p=0.048).
Conclusions
Given the results of the study, we provided major findings regarding iron deficiency anemia in pregnant women in relation to gestational age, birth weight, APGAR score and the presence of neonatal pathologies. Although the prevalence of iron deficiency anemia in pregnant women was quite high in the study group, low hemoglobin values during pregnancy did not significantly influence the gestational age and newborn weight, but they were significantly correlated with difficult adaptation to extrauterine life (APGAR score) and with newborn pathologies (prolonged jaundice, anemia, respiratory distress). At the same time, preterm infants required prolonged hospitalization to receive adapted artificial feeding, being deprived of the benefits of natural feeding. Thus, we consider that prophylaxis of iron deficiency anemia in pregnant women remains of major practical importance, with a positive impact also on the newborn.
Acknowledgements. This article contains the results of a study carried out for a dissertation. The authors thank all the women who participated in the study, as well as the authorities of the “Sf. Ioan cel Nou” County Emergency Clinical Hospital, Suceava, for their cooperation in the research.
Authors’ contribution
O.A. – study design, data interpretation, critical revision and editing of manuscript, final approval for publication.
P.M. – study design, research implementation, drafting of manuscript, data collection, statistical analysis, data interpretation, final approval for publication.
B.S. – study design, study validation and supervision, critical review of manuscript, final approval for publication.
Conflict of interests: The authors declare no conflict of interests.
Bibliografie
-
Whitney E, Rolfes SR. Understanding Nutrition. 11th edition. Thomson-Wadsworth. 2008.
-
Society of Obstetrics and Gynaecology of Romania. Clinical guidelines of obstetrics and gynaecology 2007-2013. Iron deficiency anaemia in pregnant women.
-
Graur M, et al. Guide to healthy eating. Iaşi: Performantica Publishing House. 2006.
-
Bendich A, Deckelbaum RJ. Preventive Nutrition Throughout the Life Cycle – A Cost-Effective Approach to Improved Health. In: Bendich A, Deckelbaum RJ. Preventive Nutrition: The Comprehensive Guide for Health Professionals. 3rd Ed. Humana Press. 2005, 901-922.
-
Byrd -Bredbenner C, Beshgetoor D, Moe G, Berning J. Wardlaw’s Perspectives in Nutrition. 8th edition. McGraw-Hill. 2009.
-
Boccio J, Iyengar V. Iron Deficiency Causes, Consequences, and Strategies to Overcome This Nutritional Problem. Biol Trace Elem Res. 2003;94:1-31.
-
Sabina S, Iftequar S, Zaheer Z, Khan MM, Khan S. An Overview of Anemia in Pregnancy. JIPBS. 2015;2(2):144-151.
-
Ziegler J, Mobley C. Pregnancy, Child Nutrition, and Oral Health. In: Touger-Decker R, et al. (eds.): Nutrition and Oral Medicine. Nutrition and Health. Springer. 2014, 19-37.
-
Malhotra N, Upadhyay RP, Bhilwar M, Choy N, Green T. The Role of Maternal Diet and Iron-folic Acid Supplements in Influencing Birth Weight: Evidence from India’s National Family Health Survey. J Trop Ped. 2014;60(6):454-460.
-
Athiyarath R, Shaktivet K, Abraham V, et al. Association of genetic variants with response to iron supplements in pregnancy. Genes Nutr. 2015;10(4):474.
-
Derbyshire E. Iron deficiency anaemia in pregnancy – what are the solutions?. Nutrition & Food Science. 2010;40(6):598-607.
-
Papadopoulou E, Stratakis N, Roumeliotaki T, et al. The effect of high doses of folic acid and iron supplementation in early-to-mid pregnancy on prematurity and fetal growth retardation: the mother-child cohort study in Crete, Greece (Rhea study). Eur J Nutr. 2013;52:327-336.
-
Ribot B, Aranda N, Viteri F, Hernandez-Martinez C, Canals J, Arija V. Depleted iron stores without anaemia early in pregnancy carries increased risk of lower birthweight even when supplemented daily with moderate iron. Hum Reprod. 2012;27(5):1260-1266.
-
Ministry of Health. Suceava Public Health Directorate. Pregnant Woman’s Booklet. 2005.

Diagnostic challenges in recurrent respiratory infections in children – the vascular ring. A case report
Bianca Raluca Mateescu, Alina Grama, Georgiana Laura Cioancă, Simona Căinap, Tudor Lucian Pop
Infecţiile respiratorii recurente sunt cauze frecvente de solicitare a consultului medical în populaţia pediatrică. Cauzele acestor manifestări sunt foarte variate, astfel încât o încadrare core...
Acute liver failure associated with recent SARS-CoV-2 infection in a pediatric patient – case report
Georgiana Laura Cioancă, Alina Grama, Luciana Petrescu, Simona Căinap, Bianca Raluca Mateescu, Gabriel Benţa, Bogdan Bulata, Tudor Lucian Pop
Insuficienţa hepatică acută (IHA) la copil este o patologie rară, dar severă, caracterizată prin coagulopatie şi modificări de lab...
Sleep-related breathing disorders in the pediatric patient with Prader-Willi syndrome
Sorina Chindriş, Gabriela Vlad, Ana Maria Daviţoiu, Eugenia Buzoianu, Mirela Iancu, Iulia Ţincu, Ioana Adriana Ghiorghiu, Monica Albert, Andrei Zamfirescu, Doina Anca Pleşca
Sindromul Prader-Willi (PWS) este o boală genetică rară, întâlnită cu o incidenţă de 1:15000 de nou-născuţi, identificată la to...
Sleep-related breathing disorders in the pediatric patient with Prader-Willi syndrome
Sorina Chindriş, Gabriela Vlad, Ana Maria Daviţoiu, Eugenia Buzoianu, Mirela Iancu, Iulia Ţincu, Ioana Adriana Ghiorghiu, Monica Albert, Andrei Zamfirescu, Doina Anca Pleşca
Sindromul Prader-Willi (PWS) este o boală genetică rară, întâlnită cu o incidenţă de 1:15000 de nou-născuţi, identificată la to...
Analiză clinică a malformațiilor arcului aortic: perspective din multiple studii de caz
Cosmin Diaconescu, Dana-Elena Mîndru, Bogdan A. Stana, Cristina Stoica, Alexandra Tincu, Tudor Tincu, Heidrun Adumitrăchioaiei, Alina-Costina Luca
Malformațiile arcului aortic sunt boli congenitale rare, care adesea se prezintă fără simptome, făcând dificilă documentarea lo...