Introduction. Epidermolysis bullosa (EB) is a genetic disease that predominantly affects the skin. Among extracutaneous manifestations, the oral and dental lesions have a significant influence on the prognosis of the patient, being able to cause a number of metabolic and immunological abnormalities.
Case report. We present the case of a female patient, aged 5 years and 2 months, suffering from bullous epidermolysis, who was hospitalized for eating difficulties. During the oral cavity examination, numerous dental caries with multiple root scars were found. The vesicular lesions were also identified on the tongue, both disorders leading to a significant difficulty in mastication and swallowing.
Conclusions. Dental abnormalities in patients with EB represent a real challenge for the dentist. This group of patients require a special dental rehabilitation plan because they have generalized episodic hypoplasia and pose a significant risk of intraoral lesions. Also, the oral manifestations of the disease can easily guide an early diagnosis.
Anomalii orale ereditare – copil diagnosticat cu epidermoliză buloasă
Hereditary oral anomalies – a child diagnosed with epidermolysis bullosa
First published: 30 noiembrie 2018
Editorial Group: MEDICHUB MEDIA
DOI: 10.26416/Orl.41.4.2018.2122
Abstract
Rezumat
Introducere. Epidermoliza buloasă (EB) este o afecţiune genetică, afectând în mod predominant pielea. Printre manifestările extracutanate, leziunile orale şi dentare au o influenţă semnificativă în prognoza pacientului, afecţiunea putând cauza anormalităţi metabolice şi imunologice.
Studiu de caz. Prezentăm cazul unei paciente în vârstă de 5 ani şi 2 luni, suferind de epidermoliză buloasă, care a fost spitalizată pentru dificultăţi de alimentaţie. În timpul examinării cavităţii orale au fost descoperite numeroase carii dentare, inclusiv cu multiple afecţiuni ale rădăcinor. Au fost identificate şi leziuni veziculoase pe limbă, ambele tulburări ducând la o dificultate semnificativă în masticare şi înghiţire.
Concluzii. Anomaliile dentare la pacienţii cu EB reprezintă o adevărată provocare pentru dentist. Acest grup de pacienţi necesită un plan special de reabilitare dentară, deoarece au hipoplazie episodică generalizată şi prezintă un risc semnificativ de leziuni intraorale. Totodată, manifestările orale ale afecţiunii pot ghida cu usurinţă spre un diagnostic precoce.
Introduction
Epidermolysis bullosa (EB) is a genetic disease with mucocutaneous damage caused by mutations in various structural proteins of the skin(1). The onset of the disease is usually in the first months after birth(2), and in time there is a systemic disorder with numerous organ and system dysfunctions(3). The general recurrence of inherited EB was assessed at 19.57 cases per 1 million live births(4) and is accompanied by high morbidity and mortality(5).
The spectrum of extracutaneous manifestations is wide, being mainly determined by the damage to the respiratory, gastrointestinal, urogenital and metabolic systems(6). These include oral and dental abnormalities. Peri- and intraoral blisters, ankyloglossia, microstoma, dental enamel hypoplasia, tooth dysplasia, excessive caries, premature tooth loss, and tooth misalignment have been described(6).
We present the case of a patient diagnosed with EB, suffering from numerous mouth injuries, dental abnormalities and severe swallowing disturbances.
Case report
We present the case of a female patient, aged 5 years and 2 months, who was admitted in a pediatric hospital from Bucharest for eating difficulties. From her personal physiological antecedents, she is the second-born child of the family, born in term, with a birth weight of 2300 g, Apgar score 8, and good postnatal evolution. From the age of about 3 years old, the child begins to experience bloody skin lesions that require numerous admissions to pediatric and dermatology hospitals. The heredo-collateral antecedentes highlights the presence in the mother’s childhood of non-characteristic skin rashes, which had not been diagnosed. The father and elder sister have no significant pathological history.
General clinical examination: on the skin of the upper limb, there are present vesicular-bullous type lesions, isolated or clustered, sometimes denuded and with signs of superinfection. The upper limbs also present onychodistrophy lesions and even nail amputation. Moreover, scars and sinuses can be found here, especially in the areas surrounding the interphalangeal joints. All these lesions are accentuated and expanded by exposure to heat.
At the facies level, scar tissue areas with extensive localization and numerous sinuses can be observed, along with microstoma. The functional examination reveals severe functional disorders of mastication and swallowing. Feeding is difficult, even though food is soft and liquid.
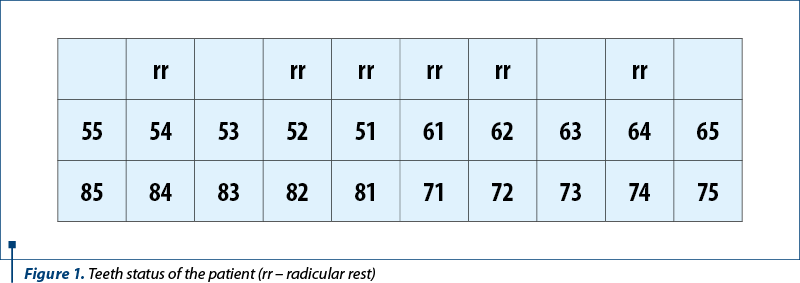
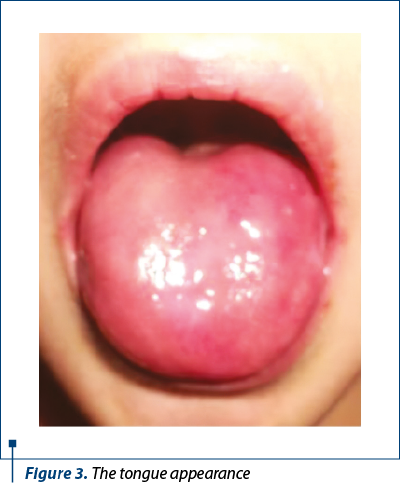
At the level of the oral cavity there are structural abnormalities leading to early caries with rapid evolution to root remnants. The patient has temporary dentition, with the dental status shown in Figure 1. The carious activity is increased, with the patient showing radical scrap at the level of: 54, 52, 51, 61, 62, 64, and extended carious processes at the level of 84 and 74 crowns. Also, hypoplastic enamel areas with a thin rough layer can be observed at the level of 53 and 63 crowns (Figure 2). The lingual mucosa has numerous vesicles, the tongue gaining a depressed appearance (Figure 3).

Discussion
Although the main manifestations in bullous epidermolysis are cutaneous, extracutaneous damage should not be neglected, significantly influencing the quality of life and survival. Oral and dental involvement is an important complication for most patients with EB, leading to a number of metabolic abnormalities as a result of eating difficulties(7). In a meta-analysis published in 2012, Kramer et al.(8) set out some guidelines regarding oral health care in patients with EB.
For patients diagnosed from birth, it is recommended that the first dental consultation be performed at the age of 3-6 months, to prevent early complications. Regular oral hygiene using a small and soft toothbrush is important for the prevention of tooth decay(8). Furthermore, the professional use of an ultrasonic scaler, polish, and high-dose fluoride varnish at frequent intervals are recommended for all epidermolysis bullosa patients(8,9). A good oral hygiene associated with an intense oral examination program will lead to a good nutritional status, to a decreased incidence of oral cavity infections, to an increased self-esteem by improving aesthetics, and also to the achievement of proper phonetics(8).
In the case of already installed lesions, dental treatment should be done as early as possible, in some situations including extraction and replacement of the teeth(9). In these patients, consideration should be given to the use of soft dressings and the careful positioning of the tube of aspiration in order not to cause injuries both intraoral and extraoral(10).
As in the case of our patient, an important complication is swallowing due to strictures and lesions at the esophageal level. These are frequently described in the literature and contribute significantly to the worsening of nutritional status and increased morbidity and mortality(11).
Conclusion
Dental abnormalities in patients with EB represent a real challenge for the dentist. This group of patients require a special dental rehabilitation plan because they have generalized enamel hypoplasia and pose a significant risk of intraoral lesions.
Compliance with ethics requirements:
The authors declare no conflict of interest regarding this article.
The authors declare that all the procedures and experiments of this study respect the ethical standards in the Helsinki Declaration of 1975, as revised in 2008(5), as well as the national law. The informed consent was obtained from the patient included in the study.
There was no funding for this study.
Conflict of interests: The authors declare no conflict of interests.
Bibliografie
- Intong LR, Murrell DF. Inherited epidermolysis bullosa: new diagnostic criteria and classification. Clin Dermatol. Jan-Feb 2012; 30(1):70-77.
- Horn HM, Tidman MJ. The clinical spectrum of dystrophic epidermolysis bullosa. Br J Dermatol. Feb 2002; 146(2):267-274.
- Cohn HI, Teng JM. Advancement in management of epidermolysis bullosa. Curr Opin Pediatr. Aug 2016; 28(4):507-516.
- Fine JD. Epidemiology of Inherited Epidermolysis Bullosa Based on Incidence and Prevalence Estimates From the National Epidermolysis Bullosa Registry. JAMA Dermatol. Nov 1 2016; 152(11):1231-1238.
- Uitto J, McGrath JA, Rodeck U, Bruckner-Tuderman L, Robinson EC. Progress in epidermolysis bullosa research: toward treatment and cure. J Invest Dermatol. Jul 2010; 130(7):1778-1784.
- Laimer M, Prodinger C, Bauer JW. Hereditary epidermolysis bullosa. J Dtsch Dermatol Ges. Nov 2015; 13(11):1125-1133.
- Zidorio AP, Dutra ES, Leao DO, Costa IM. Nutritional aspects of children and adolescents with epidermolysis bullosa: literature review. An Bras Dermatol. Mar-Apr 2015; 90(2):217-223.
- Kramer SM, Serrano MC, Zillmann G, et al. Oral health care for patients with epidermolysis bullosa – best clinical practice guidelines. Int J Paediatr Dent. Sep 2012; 22 Suppl 1:1-35.
- Elluru RG, Contreras JM, Albert DM. Management of manifestations of epidermolysis bullosa. Curr Opin Otolaryngol Head Neck Surg. Dec 2013;21(6):588-593.
- Korolenkova MV. Dental treatment in children with dystrophic form of epidermolysis bullosa. Stomatologiia (Mosk). 2015; 94(2):34-36.
- Fine JD, Mellerio JE. Extracutaneous manifestations and complications of inherited epidermolysis bullosa: part I. Epithelial associated tissues. J Am Acad Dermatol. Sep 2009; 61(3):367-384; quiz 385-366.
Articole din ediţiile anterioare
Carcinom spinocelular dezvoltat pe leziuni de lichen plan oral – prezentare de caz şi revizuirea literaturii de specialitate
Oral lichen planus (OLP) is a relatively common chronic inflammatory disease that involves the oral mucous membranes.