Diagnosticul prenatal al blocului atrioventricular fetal
Prenatal diagnosis of fetal atrioventricular heart block
Abstract
Fetal atrioventricular heart block (FAVB) is the most commonly observed type of fetal bradycardia, and is potentially life-threatening. This condition occurs when there is a blockage in the electrical pathway between the atria and the ventricles of the heart, which can cause the heart to beat too slow or irregularly. This can lead to a range of complications, including heart failure, stroke and even death. This paper presents some interesting pictures of FAVB in cases associated with autoimmune diseases and also some normal recordings in the hope of a better understanding of this condition. We intend to provide some usefully visual information for clinicians involved in the management of fetal cardiovascular disorder. The correct diagnosis using the right ultrasound tools and the referral for an echocardiography are key factors for a proper management of this condition.Keywords
fetal atrioventricular heart blockprenatal diagnosiscausesfetal echocardiographyM-modeRezumat
Blocul atrioventricular (BAV) fetal este una dintre cele mai frecvente tipuri de bradicardie fetală. Este produs de un blocaj în transmiterea semnalului electric dintre atrii şi ventriculi, ceea ce duce la un ritm cardiac mult prea lent sau iregulat. Blocul atrioventricular fetal poate cauza o serie de complicaţii, incluzând insuficienţă cardiacă şi chiar moarte fetală intrauterină. Articolul prezintă câteva cazuri interesante de BAV fetal la paciente care prezintă patologie autoimună, în scopul unei mai bune înţelegeri a acestei patologii şi al unui diagnostic prenatal corect. Scopul articolului este de a aduce informaţii utile privind diagnosticul ecografic al acestei patologii. Diagnosticul corect, folosind tehnicile potrivite, şi direcţionarea pacientei către un centru de specialitate reprezintă prima etapă în managementul adecvat al acestei patologii, care poate pune în pericol viaţa fătului.Cuvinte Cheie
bloc atrioventricular fetaldiagnostic prenatalcauzeecocardiografie fetalăM-modeIntroduction
Fetal atrioventricular heart block (FAVB) is a rare congenital heart condition that affects the electrical signals in the heart. The condition occurs when there is a blockage in the electrical pathway between the atria and the ventricles of the heart, which can cause the heart to beat too slow or irregularly. This can lead to a range of complications, including heart failure, stroke and even death(1).
FAVB is typically diagnosed during pregnancy, using fetal echocardiography, a type of ultrasound that allows doctors to assess the structure and function of the fetal heart. The condition can also be detected after birth, using a variety of diagnostic tests, including electrocardiography (ECG) and cardiac catheterization(2). Ultrasound examination must include the M-mode recording and Power wave Doppler for a correct diagnosis. M-mode ultrasound (also called motion-mode imaging) does not yield full frame images per se, but rather one selected image line is rendered as a function of time. This is used for displaying motion of – for example – the periodic movement of heart valves. Any abnormalities or temporal variations can be directly seen as an image on the screen(4).
The treatment of FAVB depends on the severity of the condition and on the gestational age of the fetus. In some cases, medications may be used to help regulate heart’s rhythm and improve blood flow. In more severe cases, surgery may be necessary to repair the electrical pathway between the atria and the ventricles(3). Steroids are often used. Care should be taken in these cases, as they can further affect the heart, causing pericardial effusion, left ventricular enlargement and poor contractility(5).
In conclusion, FAVB is a rare but serious condition that can have significant consequences for the developing fetus. Early diagnosis and treatment are essential for improving outcomes and for preventing complications. Further research is needed to better understand the causes and the management of FAVB.
Congenital heart block is a condition that occurs when the electrical signals that control the heart’s rhythm are disrupted. This can be caused by a variety of factors, including:
Genetic factors. Congenital heart block can be caused by certain genetic conditions, such as lupus, rheumatoid arthritis or Sjögren’s syndrome, which can affect the development of the heart.
Infections. Infections during pregnancy, such as rubella or cytomegalovirus, can cause congenital heart block.
Medications. Some medications, such as certain types of heart medication or certain types of antibiotics, can increase the risk of congenital heart block.
Environmental factors. Exposure to certain environmental toxins, such as tobacco smoke or some chemicals, during pregnancy can increase the risk of congenital heart block. It’s important to note that, in many cases, the cause of congenital heart block is unknown(6).
Interesting images
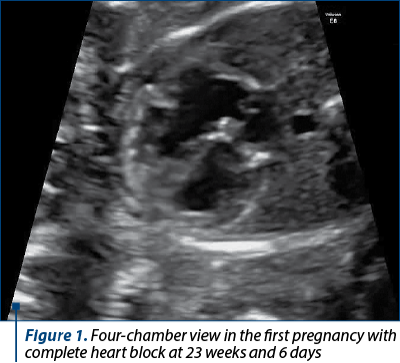
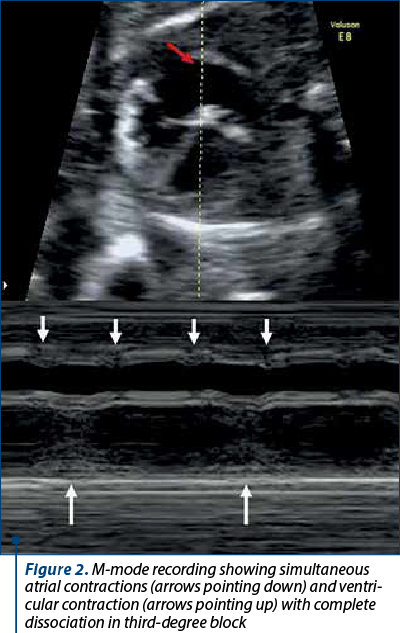
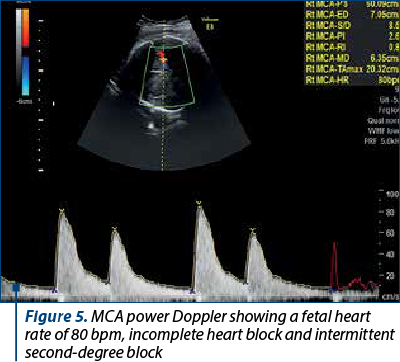
We present the case of a 30-year-old female patient with Sjögren’s syndrome and anti-RO antibodies present. In her first pregnancy, she had termination at 24 weeks for complete heart block (Figures 1 and 2).
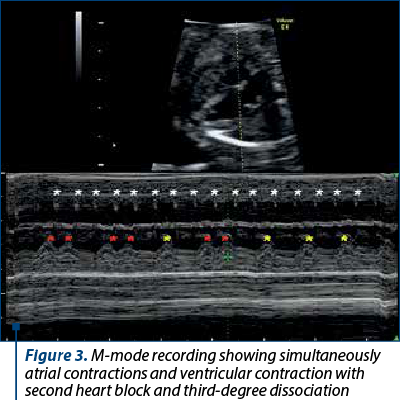
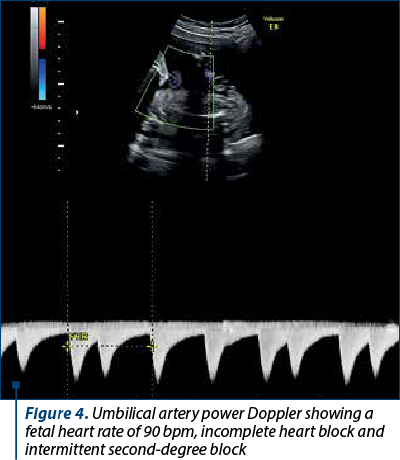
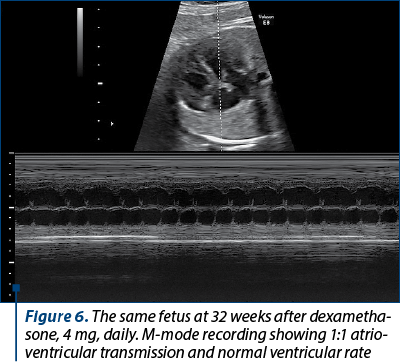
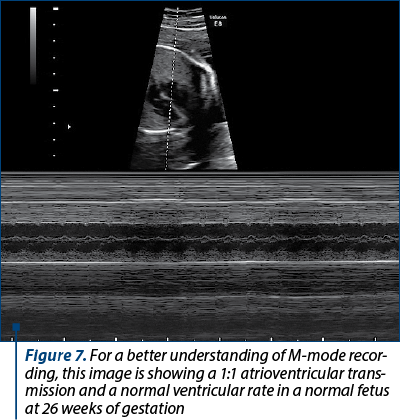
This is her second pregnancy. Unfortunately, even with hydroxychloroquine prophylaxis at 22 weeks, second- and third-degree block was detected (Figures 3-7).
Conclusions
It is extremely important to recognize the condition for a correct management plan. Complete atrioventricular block leads to complete dissociation of the atrial and ventricular activity as a result of the damage in the atrioventricular conduction pathways. In patients with third-degree atrioventricular block, the atrial frequency is in the normal range, but the ventricular rate can be lower than 50 beats per minute, usually between 50 and 80 beats/minute. The ultrasound findings in fetal life include ventricular dilatation, reduced ejection fraction, echogenic endocardium located in the left ventricle affecting the mitral valve papillary muscles, and atrioventricular valve causing valve dysfunction. After the suspicion or diagnosis, the patient must be referred for an echocardiography for the exclusion of additional findings and for treatment. The use of M-mode recoding is essential for the diagnosis and it should be used alongside power wave Doppler and 2D imaging of the heart.
Conflict of interests: The authors declare no conflict of interests.
Bibliografie
-
Pruetz JD, Miller JC, Loeb GE, Silka MJ, Bar-Cohen Y, Chamait RH. Prenatal diagnosis and management of congenital complete heart block. Birth Defects Res. 2019:111(8):380-8.
-
Simpson J, Vita Z, Miller Owen I. Fetal Cardiology: a practical approach to diagnosis and management. London: Springer, 2019.
-
Hongyo L, Tang C, Qiao L, Zhou K, Li Y. Prenatal management strategy for immune-associated congenital heart block in fetuses. Front Cardiovasc Med. 2021;8:644122.
-
Mertens LL, Rigby ML, Horowitz ES, Anderson RH. Cross Sectional Echocardiographic and Doppler Imaging. In: Paediatric Cardiology (3th Ed), Churchill Livingstone. 2010:313-39.
-
Cimpoca-Raptis B, Ciobanu AM, Gică N, Scutelnicu AM, Bouariu A, Popescu M, Panaitescu AM. Recurrent congenital heart block due to maternal anti-ro antibodies: successful prevention of poor pregnancy outcome with Hydroxychloroquine and added Dexamethasone. Reprod Med. 2022:3(1):36-41.
-
Hansahiranwadee W. Diagnosis and management of fetal autoimmune atrioventricular block. Int J Womens Health. 2020;2020(12):633-9.

December 2022 – February 2023 Calendar
December 2022 – February 2023 Calendar...
Senologie benignă
La Editura Medicală a apărut lucrarea Senologie benignă (455 de pagini). Autorul, dr. Ştefan Voiculescu, promovează insistent recomandările de raportare standardizată (terminologia ghidurilor internaţionale, scorul BIRADS, categorii nosologice, algoritmi de monitorizare şi tratament, timpi op...
Caracteristicile neonatale în malformaţiile urologice congenitale – experienţa noastră
Daniela-Mariana Manea (Lascoschi), Mihai-Daniel Dinu, Romina-Marina Sima, Liana Pleș, Anca Daniela Stănescu
Congenital defects of the kidney and urinary tract represent approximately 20-30% of all malformations identified in the prenatal period(1). These defects can be unilateral or bilateral, and sometimes...
Mortalitatea maternă şi fetală în rândul pacientelor adolescente
Ana Veronica Uzunov, Daniela-Cătălina Meca, Monica-Mihaela Cîrstoiu
Adolescence is defined by World Health Organization (WHO) as the period of transition from childhood to adult lifetime in the population aged between 10 and 19 years old(1,2). The incidence of births among adolescents is...
Diabetul gestaţional – o provocare obstetricală, neonatală şi postnatală
Oana Dorobanţu, Andrei Vasilăţeanu
In recent decades, the demographics of pregnant women have changed, with an increase of women giving birth at an older age and which, associated with the increase of obesity, has led to a rise in the prevalence of gestat...