Malformaţii cardiace fetale detectabile pe secţiunea de trei vase
Congenital heart diseases that are detectable using the three-vessel view
Abstract
Congenital heart defects are the most common congenital malformation found in fetuses. The majority of ultrasound screening protocols recommend as mandatory the following views for the examination of the fetal heart: 4 chamber and ventricular outflow tracts. The 3-vessel view alongside its variant, the 3-vessel trachea view, are considered optional planes for routine screening. A series of congenital heart defects are mainly visible and detectable in these two views, so including these views in the screening protocol may be beneficial. We identified three types of congenital heart defects that are usually detected using the 3-vessel and 3-vessel trachea views: aortic coarctation, right aortic arch, and the persistence of left superior vena cava. All three malformations had a characteristic appearance on the aforementioned views. Taking into account the role they have in detecting these specific congenial heart defects, the 3-vessel and 3-vessel trachea view prove their role in evaluating the fetal heart and may improve the detection of ultrasound screening.Keywords
3-vessel viewconotruncal malformationscongenital heart defectsaortic coarctationright aortic archleft superior vena cavaRezumat
Defectele cardiace congenitale reprezintă cel mai frecvent tip de malformaţie congenitală întâlnită la făt. Majoritatea protocoalelor de screening ecografic recomandă ca obligatorii următoarele imagini sau secţiuni ecografice pentru evaluarea cardiacă: imaginea de 4 camere, imaginile cu tracturile de ejecţie a ventriculilor. Imaginea de 3 vase, alături de varianta sa, imaginea de 3 vase şi traheea, sunt considerate secţiuni opţionale pentru screeningul ecografic. O serie de defecte cardiace congenitale sunt vizibile şi detectabile pe aceste imagini, astfel încât includerea lor în protocolul de screening poate fi benefică. Am identificat trei tipuri de malformaţii care sunt detectate, de obicei, folosind secţiunea de 3 vase şi secţiunea de 3 vase şi traheea: coarctaţia de aortă, arcul aortic drept, persistenţa de venă cavă superioară stângă. Toate cele trei malformaţii au un aspect caracteristic pe secţiunile ecografice menţionate anterior. Având în vedere rolul pe care îl au în detectarea acestor malformaţii cardiace, imaginea de 3 vase, alături de imaginea de 3 vase şi traheea îşi dovedesc rolul pe care îl au în evaluarea cardiacă fetală şi ar putea îmbunătăţi rata de detecţie a screeningului ecografic.Cuvinte Cheie
imaginea de 3 vasemalformaţii conotruncaledefecte cardiace congenitalecoarctaţie de aortăarc aortic dreptvenă cavă superioară stângăIntroduction
Congenital heart defects (CHD) are the most frequent type of malformations found in fetuses. The incidence varies between 12-14 per 1000 live births, but can be as high as 50 per 1000 live births if less severe CHD such as the persistence of left superior vena cava are taken into account(1,2). Although some of them may be only minor, they must not be overlooked, as they can be a sign of a genetic disease or of more severe malformations. The majority of ultrasound screening protocols state only the 4-chamber and ventricular outflow views as mandatory, but encourage the visualization of other views used in fetal echocardiography when possible(3-5). The 3-vessel view (3VV) and its slightly more cephalic variant, the 3-vessel trachea view (3VT), are usually considered optional scanning planes in screening protocols. Nonetheless, a series of CHD are visible mainly on these two planes, so by making them mandatory screening planes, the rate detection for CHD might be increased. We set out to describe the ultrasound elements that define the normal 3VV and 3VT views. Also, we will present three types of CHD that are detected using only or mainly these two planes.
Method
To define the normal ultrasound appearance of the 3VV and 3VT views, we used the original articles of Yoo et al. and Yagel et al.(6,7) for documentation, who described these views, and also the 2013 updated ISUOG guideline(4). Although there are numerous articles in literature on this topic, the basic definition and ultrasound characteristics of the two views have remained largely unchanged.
Regarding the CHD that are detected with the help of the 3VV and 3VT, we analyzed the cases included in the PhD thesis “Secţiunile 4 camere şi 3 vase – rol în evaluarea cardiacă fetală”. These cases were scanned by ultrasound and collected by Dr. Doru Herghelegiu and Dr. Cătălin Gabriel Herghelegiu between 2016 and 2019. The gestational age of the fetuses varied between 20 and 30 weeks. The ultrasound examinations were performed using Voluson 730Expert, E8 ultrasound machines, and transabdominal curvilinear transducers were used. Only those cases with abnormal 3VV and/or 3VT views, but normal 4 chamber and outflow tract views were included.
Results and discussion
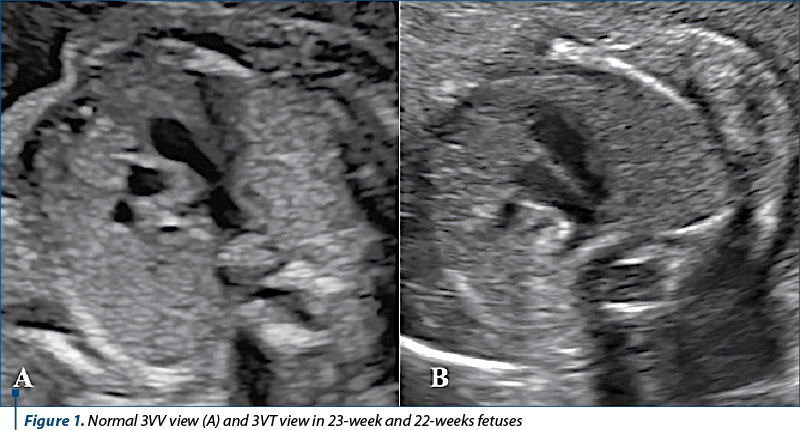
The 3VV is a transverse section of the thorax at the level of the upper mediastinum. To avoid slightly oblique planes, it is recommended that only one rib should be visible on each side of the thorax. From right to left and from posterior to anterior, 3 vessels are observed: the superior vena cava, the ascending aorta, and the pulmonary trunk continuing posteriorly with the ductus arteriosus (Figure 1A). The 3 vessels are arranged in a straight line and from small to large, the inferior vena cava being the smallest and the pulmonary trunk being the largest. The 3VT is located slightly more cephalic and has the advantage of allowing the visualization of a transverse section of the aortic arch. In this plane, the aortic arch and ductus arteriosus converge towards the descending aorta and form a characteristic “V” sign and both vessels are similar in dimension (Figure 1B). Also, the relationship of the two arteries with the trachea can be assessed in this view. Normally, they are both situated to the left of the trachea.
A total of 8 cases of CHD with abnormal 3VV and/or 3VT views, but normal 4 chamber and outflow tract views were identified. Regarding the types of CHD, there were encountered the following: three cases of aortic coarctation (AoCo), two cases of right aortic arch (rAo), three cases of persistent left superior vena cava (LSVC).
Aortic coarctation
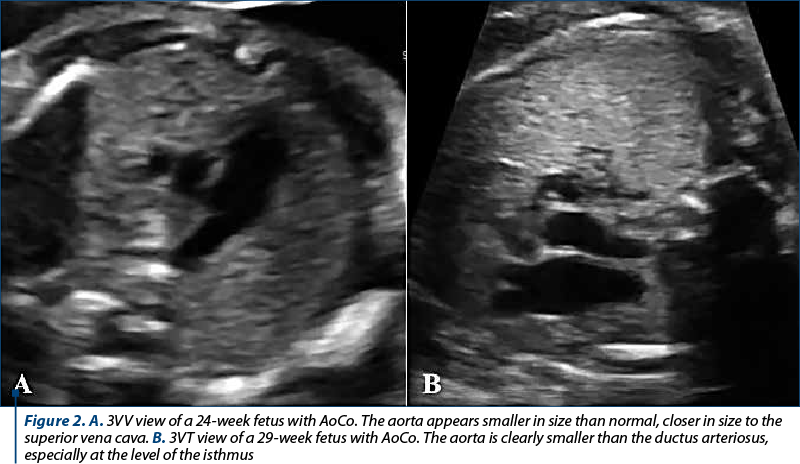
Only 3 cases of the total of 9 cases of AoCo identified had a normal 4-chamber view (the ventricles having roughly the same size) and were included in the study. In only one case, the 3VV view was abnormal, with the diameter of the ascending aorta being slightly diminished in comparison with the pulmonary trunk and having a dimension similar to that of the superior vena cava (Figure 2A). This is because only in severe cases of AoCo the whole aortic arch is narrowed, most of the times only the distal portion being affected. On the 3VT, all three cases had an abnormal appearance, with the aortic arch being considerably stenotic in the isthmus portion and considerably smaller than the ductus arteriosus (Figure 2B). It is recommended to orient the thorax with the spine at 3 or 9 o’clock, in order to avoid ultrasound shadowing from the vertebra and to better assess the size of the aorta and ductus arteriosus. Although the diagnosis of aortic coarctation is best to be established on sagittal planes, which allow the visualization of the whole aortic arch, these planes are often hard to be obtained, especially near the end of the pregnancy, because of the fetal position and the ultrasound shadowing produced by the ossified vertebra and scapula. Thus, in these suboptimal (examination) conditions, the 3VT can be a valuable tool in diagnosing AoCo, a pathology that in some cases evolves and aggravates towards the end of the pregnancy.
Right aortic arch
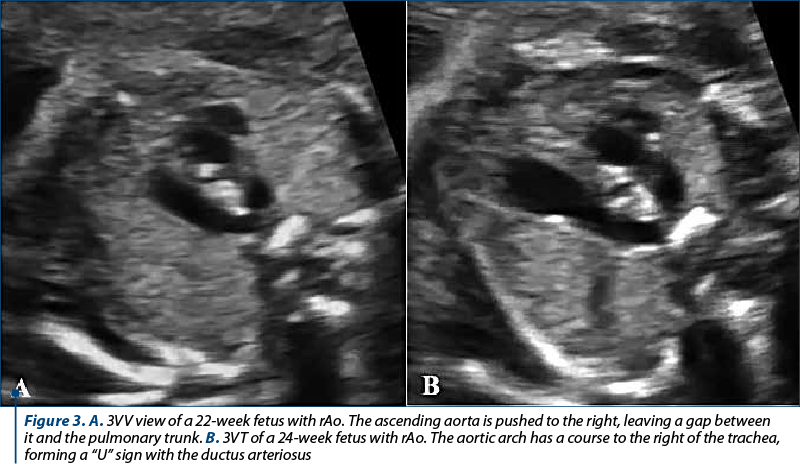
The two isolated rAo cases displayed a characteristic pattern on the ultrasound images. On the 3VV, the ascending aorta appears pushed to the right, into the superior vena cava, being further away than normal from the pulmonary trunk (Figure 3A). The ductus arteriosus, in its distal region, has a slightly abnormal course to the right, ending near the midline and not to the left of the vertebra, as it should be normal. On the 3VT, the diagnosis becomes clearer, as the aortic arch is located to the right of the trachea (Figure 3B). Thus, the aorta and the ductus arteriosus form a “U” sign, encircling the trachea, and not the typical “V” sign seen in normal cases.
Left superior vena cava (LSVC)
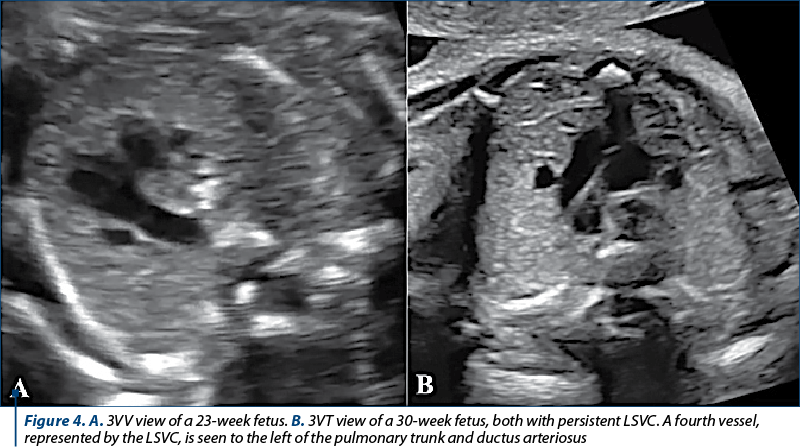
The persistence of the LSVC can be an isolated CHD or it can be a sign for a much more complex CHD or even a genetic disease. A total of three cases of isolated persistence of LSVC were found in the analyzed cases. Both the 3VV and the 3VT views were abnormal, as a small forth vessel, represented by the LSCV, could be observed (Figure 4). The LSVC is located to the left of the pulmonary trunk and ductus arteriosus. The diagnosis becomes more obvious after the second half of the second trimester, when the vessel grows in size and is easier to spot.
Conclusions
The 3VV and 3VT views are transverse planes at the level of the upper mediastinum and are easy to be obtained during routine ultrasound screening. There are a series of ultrasound elements that define the normal appearance of the two views. Both the 3VV and 3VT represent a valuable method of detecting CHD, especially those that involve the great vessels(8). The current study highlights a series of CHD (AoCo, rAO, LSCV) that are detectable using these two views, as the views recommended by screening protocols (4-chamber view and ventricular outflow tract views) are normal. Still, for a complete evaluation of the fetal heart, all the transverse planes aforementioned and also sagittal ones are recommended to be obtained.
Conflict of interests: The authors declare no conflict of interests.
Bibliografie
-
Hoffman JIE, Kaplan S. The incidence of congenital heart disease. J Am Coll Cardiol. 2002; 39:1890–900.
-
Van der Bom T, Zomer AC, Zwinderman AH, Meijboom FJ, Bouma BJ, Mulder BJM. The changing epidemiology of congenital heart disease. Nat Rev Cardiol. 2011; 8:50–60.
-
Pelinescu-Onciu D, Vlădăreanu R, Stamatian F, Calomfirescu MV, Mărginean C, Mureşan D, Pleş L, Ceauşu I, Tudorache Ş, Iliescu D, Veduţă A. Examinarea ecografică de screening pentru anomalii de sarcină în trimestrul 2. MS, 2019.
-
ISUOG Practice Guidelines (updated): Sonographic screening examination of the fetal heart. Ultrasound Obs Gynecol. 2013; 41:348–59.
-
AIUM Practice Guideline for the Performance of Obstetric Ultrasound Examinations. J Ultrasound Med. 2013; 32:1083–101.
-
Yoo SJ, Lee Y-H, Kim ES, Ryu HM, Kim MY, Choi H-K, Cho KS, Kim A. Three-vessel view of the fetal upper mediastinum: an easy means of detecting abnormalities of the ventricular outflow tracts and great arteries during obstetric screening. Ultrasound Obstet Gynecol. 1997; 9:173–82.
-
Yagel S, Arbel R, Anteby EY, Raveh D, Achiron R. The three vessels and trachea view (3VT) in fetal cardiac scanning. Ultrasound Obstet Gynecol. 2002; 20:340–5.
-
Herghelegiu CG, Dragan I, Suciu N, Oprescu ND. A simplified protocol for congenital heart disease. 5th Congr Rom Soc Ultrasound Obstet Gynecol. 2017; 298–302.

Nefrectomie laparoscopică cu extragerea transvaginală a rinichiului. Primul caz realizat în România – premieră naţională
Titus Sorin Pătrăşcoiu, Corneliu Roşulescu, Elvira Brătilă, Ioan Prie, Laura Popa, Claudia Pătrăşcoiu, Narcis Copca
Introducere şi obiectiv. Prezentăm cazul unei femei de 32 de ani care s-a prezentat în departamentul nostru de la Spitalul Clinic ...
Caracteristicile neonatale după transfer de embrioni fresh sau congelaţi la paciente normogonadotrope, tinere şi sănătoase
Annamaria Virginaş, Bogdan Cârstea, Szidonia Koszeghi, Istvan Barna Nagy, Zolna Virginas, Tamas Korosi, Gabor Vajta
Scop. A evalua dacă transferul de embrioni congelaţi (FET) are efecte benefice asupra greutăţii nou-născutului, comparativ cu tran...
Diagnosticul adenomiozei uterine la pacientele de vârstă reproductivă
Livia Cosma, Corina Gică, George Iancu, Radu Botezatu, Gheorghe Peltecu, Anca Maria Panaitescu, Nicolae Gică
Adenomioza uterină este o patologie ginecologică ce este caracterizată de prezenţa insulelor ectopice de ţesut endometrial în miometru. Această boală afectează 20% dintre femeile de vârstă reproduc...
Tumoră spinală cervicală asociată sarcinii
Oana Bodean, Mirela Moarcăş, Diana Ioana Voicu, Octavian Munteanu, Luciana Grozavu-Arsene, Florina Păuleț, Monica-Mihaela Cîrstoiu
Tumorile spinale sunt rar întâlnite în sarcină, dar atunci când sunt extinse, pot cauza probleme grave prin efectele neurologice rapid progresive date de compresia medulară. Tumorile cu celule Schw...
Pitiriazisul rozat în timpul sarcinii – ce ar trebui să ştie obstetricienii?
Anca A. Simionescu
Pitiriazisul rozat (PR) este o boală eruptivă cutanată care apare frecvent în sarcină. Lucrarea abordează diagnosticul şi tratamentul pe care ar trebui să le cunoască obstetricienii în privinţa acestei patologii. PR apare ca o erupţie eritemato-nepruriginoasă, de obicei localizată pe torace şi umeri, sub fo...