Tratamentul leziunilor dentare cervicale în sarcină
Treatment of cervical dental lesions in pregnancy
Abstract
In the daily practice of dental medicine, we have been frequently faced with the need for dental treatments in pregnant woman, whether it is the management of dental caries or the prophylaxis of gingivitis. The approach of the restorative treatment of the cervical dental lesions in pregnancy is conditioned by a multitude of aspects related to the physiological particularities which have resonated directly in the oral cavity. Of these, the most important factors that must be taken in consideration during the dental treatment are: the presence of pregnancy gingivitis, also of the dentin hypersensitivity and hyperesthesia; the psychoemotional status of the woman, in association with the aesthetic aspect, strongly requested by the modern society during the pregnancy period; the need to use local anesthetic substances; the longevity in the oral cavity of the restoration performed on the pregnant woman; the important local and general influence of the treatment of this type of lesions on the harmonious course of the pregnancy period.Keywords
pregnancycervical dental lesiondirect restorationRezumat
În practica de medicină dentară ne confruntăm frecvent cu necesitatea tratamentelor stomatologice la femeia însărcinată, fie că este vorba despre managementul unor leziuni carioase sau despre profilaxia gingivitei. Abordarea tratamentului restaurator al leziunilor cervicale dentare în sarcină este condiţionată de o multitudine de aspecte legate de particularităţile fiziologice, care au răsunet direct în cavitatea orală. Dintre acestea, factorii cei mai importanţi care trebuie luaţi în considerare în cursul tratamentului stomatologic sunt: prezenţa gingivitei de sarcină, precum şi a hipersensibilităţii şi hiperesteziei dentinare accentuate; statusul psiho-emoţional al femeii, în asociere cu aspectul estetic, o cerinţă a societăţii moderne şi în perioada de graviditate; necesitatea utilizării substanţelor anestezice locale; longevitatea în cavitatea bucală a restaurării efectuate la femeia însărcinată; influenţa locală şi generală a tratamentului acestui tip de leziuni asupra parcursului armonios al perioadei de sarcină.Cuvinte Cheie
sarcinăleziune dentară cervicalărestaurare directăIntroduction
Dental treatments in pregnant women are an absolute necessity. Today, they can and should be performed, knowing that the evolution of materials and techniques in the field of dental medicine is explosive and that it confers safety and predictability for the results. The exceptional progress of adhesive dental domain and the stunning properties of resin composites allow dental practitioners to perform direct restorations that until recently were considered impossible. In fact, the evolution of enamel-dentin adhesion has allowed us to achieve amazing, fast, ultra-conservative results, without the help of the dental technique laboratory by simply having available dental materials to faithfully reproduce the dental anatomy. This aspect is particularly important, considering the physiological particularities of the pregnant woman(1).
Cervical dental lesions
The cervical dental lesions are located in the cervical area of the tooth, at or next to the cementoenamel junction, being both carious and non-carious. Their progression can be either supra- or subgingival, in the latter situation with the involvement of the marginal periodontium in the clinic and the therapy of the respective lesion.
Dental caries represent the most common loss of the hard dental structure that occurs after the eruption of teeth on the dental arch and which causes a multitude of local and loco-regional complications. Due to its unsightly appearance, it also causes physiognomic dysfunctions especially when it is located in the anterior region. The onset and evolution of cervical carious lesions are favored by the fact that the cervical area of the coronal surfaces is a retention one for food debris, thus favoring the presence of bacterial dental plaque and triggering the demineralization processes of hard dental tissues(2).
Non-carious dental lesions – such as erosion and abrasion – are frequently found in the cervical area of the teeth. All these types of lesions are caused by the disappearance of hard dental tissues, both enamel and dentine, by mechanical wear or friction (in case of abrasion), by acid dissolution (in case of erosion) or by the fragmentation of enamel prisms and dentin loss (in case of abfraction)(3).
The treatment of cervical dental lesions is restorative, using direct methods, and is very important especially when one of the lesions is situated in the anterior region of the dental arch. The first-choice materials used are resin composites.
General considerations of dental treatments in pregnancy
Any dental treatment during pregnancy should take into account, first of all, the fact that the woman is in a special physiological condition of her body, with multiple general and oral cavity implications. The main objective is a correct treatment, with minimal stress for the pregnant patient. This means:
-
The treatment approach must be conservative, based on the principles of minimally invasive dentistry.
-
The operative trauma must be as low as possible regarding intensity and duration.
-
The effort to which the pregnant woman is subjected during the treatment sessions should be diminished as much as possible, by: one-session treatment is always the priority when possible and, if not, as few dental sessions as possible; short working sessions; frequent breaks during treatment; the dental chair position must be adjusted to the most comfortable position for the pregnant patient, especially in the third trimester.
-
The dentist must be patient and very understanding regardind the period of gravidity that a woman goes through, having multiple implications on the therapeutic maneuvers required, whether we are talking about practical or psychoemotional aspects(4,5).
Specific aspects of the treatment of cervical dental lesions in pregnancy
1. Pregnancy gingivitis is a physiological condition present in most women, about 50-100% of them, as a result of hormonal changes that occur in the maternal body, especially by the increased level of estrogen hormones(6).
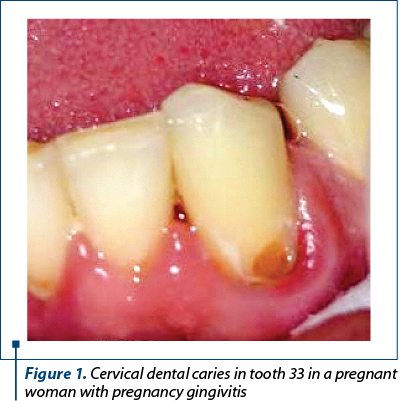
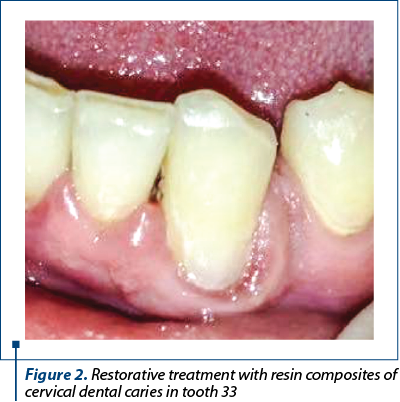
Clinically, it presents in the form of hyperplasia and gingival bleeding. The presence of bacterial dental plaque, commonly associated with cervical caries lesions, favors and maintains gingival inflammation. Thus, even a localized infection of the marginal periodontium can be triggered, in the form of a periodontal abscess. The situation is even more complicated when the pregnancy gingivitis presents in form of pregnancy epulis (pyogenic granuloma), a localized type of the gingivitis that usually needs to be removed prior to cervical lesion treatment. Therefore, the most important aspect regarding the restorative treatment of cervical lesions during pregnancy is the proximity of the area involved with the gingival tissue, which is affected by pregnancy gingivitis. Not only the evolution of carious/erosive/abrasive processes is influenced by the presence of pregnancy gingivitis, but also the therapeutic actions. Specific gingival bleeding in pregnancy gingivitis is caused by minimal contact or may even be spontaneous(7). It is the result of tissue hypervascularization and increased capillary fragility and it may prevent or limit a proper treatment with dental adhesive materials, especially when the progression of the destructive process is subgingival. In order to benefit from the excellent properties of modern adhesive materials (especially composite resins), it is necessary that the isolation of the operative field be perfect, with the absence of tissue secretions from the gingival sulcus and bleeding. Obtaining the hybrid layer during the adhesion stage, as well as the insertion of the composite are conditioned by a cavity without dentin or other kind of debris(8). The bleeding of the gingival tissue during the restoration treatment of a cervical lesion can be easily produced in all working stages: the complete removal of the altered tissues (dentin and enamel), by simply touching with rotary and/or manual instrument; cleaning the preparing cavity with strong water jet; application of dam clamps for dental isolation; air drying of the cavity after etching with phosphoric acid with high pressure air from dental unit; applying cervical celluloid matrices for restoration; insertion and adaptation at the gingival level of the restoration material when the cavity is in relation to the marginal periodontium; finishing and polishing the restoration. Hemostasis in the case of bleeding in pregnancy gingivitis is difficult, and the use of chemicals with hemostatic role is not indicated (Figure 1 and Figure 2).
2. At the cervical level, the coronary enamel layer has the smallest thickness of the entire coronary surface. Its disappearance by wear, in case of non-carious cervical lesions, leads to the exposure of dentine, with the immediate development of the dental sensitivity in the form of dental hypersensitivity and dental hyperesthesia, which are intensely perceived and little tolerated by the pregnant woman. They are also specific in cervical dental caries. Clinically, they present as a painful response to the physical, chemical and mechanical agents with which the contents of the dentin tubules come into contact(9). The pain felt by the pregnant patient causes the tooth-brushing to be avoided or incorrectly done in the involved region. The persistent bacterial dental plaque aggravates the clinical phenomena, both by the additional gingival inflammation, superimposed on the pregnancy gingivitis, as well as by accelerating the phenomena of demineralization of the dental tissues and the progression of the cervical dental lesion.
3. The psychoemotional status of the pregnant woman, also dependent on the specific hormonal changes, causes the dental pain to be frequently considered disproportionate or excessive in relation to the patient’s previous pain or sensitivity threshold. It is known that pain perception has a physical component, related to stimuli and their nerve transmission, and an individual psychic component, expressed through the perception of a painful stimulus. This aspect influences both the clinical evolution, with the appearance of hypersensitivity and of dental hysteresis, but also the maneuver of dental treatment. To the same extent, the attitude of the dentist must be supportive, patient and understanding towards the sometimes excessive reactions of the pregnant patient(10).
4. Most of the time, the presence of numerous tooth nervous terminations at the cervical level requires dental anesthesia to approach this region for therapeutic purposes. Taking into consideration the fragile sensitive psychological status frequently present in pregnant women, anesthesia becomes almost a necessity in most cases. Pregnancy involves precautions when using anesthetic substances, and the types and doses of the local anesthetics must be carefully determined in consent with gynaecologists and obstetricians. Anesthetic substances such as lidocaine or bupivacaine are among the safest to be used in pregnancy, but in general they are restricted especially in the first trimester of pregnancy, being able to interfere with the embryogenesis and organogenesis(11). Also, the anesthetic local products use is carefully supervised in the last trimester of pregnancy, when they can induce the preterm birth. As such, the only period during the nine months of pregnancy when local dental anesthesia is commonly indicated is the second trimester, when the risks are lower for the mother and fetus.
5. The topographic location of the cervical lesions causes a proximity to the dental pulp greater than in case of lesions of the same depth, on the occlusal or proximal faces. Thus, the progression of these lesions, especially when they reach the cervical dentin, can rapidly lead to the onset of irreversible pulpal inflammation, clinically characterized by acute painful symptomatology. At this stage, a root canal treatment is required, which involves multiple precautions in pregnant woman. Also, the restoration of extensive cervical lesions prevents the occurrence of coronary fractures (when the loss of hard dental substance is important) with subsequent complications related to a future restoration (when this is still possible) or the need for dental extraction in a pregnant patient(12).
6. In the modern society, pregnant women are active and present, as interested in the aesthetic aspect as in the period before pregnancy. Therefore, the restoration of the aesthetic function of the anterior area affected by cervical lesions is one of the most important and difficult challenges for the dentist, in order to restore the pleasant, natural appearance of the teeth. In this context, the proper selection of the working color shades of the dental material used for restoration is particularly important. To the same extent, the texture and the final finishing properties are equally important. Composite resins are the materials of choice for the restoration of cervical lesions. Their aesthetic possibilities give rise to a variety of therapeutic indications that continue to grow as a result of their versatility. Also, these materials are conservative regarding hard tooth structures because they are based on chemical adhesion to the enamel and dentin substrate, and do not depend on the cavity design. However, it should not be forgotten that resin composites require attention while performing work stages to achieve the desired aesthetic results(13). Following the basic principles of color determination and layering technique, we can achieve excellent results. The limitations of the use of resin composites in the cervical area are related only to the subgingival evolution of the dental caries or non-carious lesion, when using mixed restorations, in sandwich technique, with glass ionomer cement and composite.
7. The direct restorations of the cervical dental lesions must also meet, when performed in the pregnant patient, the criterion of longevity in the oral cavity. For an increased survival rate, it is necessary that the treatment principles are respected: the correct dental preparation and the working technique with the restoration materials strictly applied. For cervical lesions, the final aspect of restoration with a smooth surface, as glossy, without pores, is mandatory not only from an aesthetic point of view, but also from a prophylactic one. A very well finished and polished restoration surface, with a perfect marginal seal, prevents and/or limits the bacterial dental plaque accumulation in this physiologically retentive coronal tooth region, thus preventing the occurrence of secondary caries. In most cases, cervical lesion restorations in pregnant woman are for long term, permanent, and are not intent to be temporary restorations. Maintaining in time in good conditions the restoration carried out during gravidity is important, considering that after the pregnancy the woman faces the postnatal and breastfeeding periods, with the same impact on her life and which have their own physiological particularities, that limit to a certain extent the therapeutic approach (ex.: dental anesthetics substances, regarding breastfeeding the newborn baby)(14). Another very important aspect that contributes decisively to the success of cervical lesions over time is the right selection of resin composites or of other restorative materials according to this tooth area. A restoration with composites influences the biomechanical behavior of the respective tooth, therefore the material must possess: good abrasion resistance, filling with micro- or nanoparticles (which ensures the esthetic appearance and the possibility of perfect finishing to obtain a minimum microscopic roughness of the surface), low modulus of elasticity. This particular aspect is especially important because the pathological occlusal load produces at the cervical level flexure forces. This stress causes fractures in rigid dental structures and tends to dislocate restoration from the dental surface(15).
8. Direct restorations of cervical dental lesions in women during pregnancy have an important prophylactic and preventive role not only for the involved tooth, but also for the entire oral cavity. Once the dental treatment restores the tooth morphology and functionality and removes the painful symptoms, the patient must resume the correct habits of oral hygiene, with a proper tooth-brushing in all the regions of dental arcades. Thus, the effect is also evident in the improved clinical aspect of pregnancy gingivitis. The pregnant woman begins to use again in mastication the previously affected region and bilateral alternating food distribution has optimal effects on all the dental, bone, periodontal and temporomandibular joint structures. It thus contributes to the health of the dentomaxillary system.
9. Last but not least, the restoration of cervical dental lesions in pregnancy, by all beneficial effects provided, leads to a harmonious and beautiful course of the pregnancy period, in the general context of the holistic approach of the body.
Acknowledgements: All the authors have equal contributions for this article.
Conflict of interests: The authors declare no conflict of interests.
Bibliografie
- Giglio JA, Lanni SM, Laskin DM, Giglio NW. Oral health care for the pregnant patient. J Can Dent Assoc. 2009; 75(1):43-8.
- Schlueter N, Luka B. Erosive tooth wear – a review on global prevalence and on its prevalence in risk groups. Br Dent J. 2018; 224(5):364-70.
- Gheorghiu IM, Mitran L, Mitran M, Mironiuc-Cureu M, Stoian IM. Leziunile dentare abrazive. Medic.ro. 2013; 92(2):38-9.
- Steinberg BJ, Hilton IV, Iida H, Samelson R. Oral health and dental care during pregnancy. Dent Clin North Am. 2013; 57(2):195-210.
- Kurien S, Kattimani VS, Sriram RR, Sriram SK, Rao VKP, Bhupathi A, Bodduru RR, Patil N. Management of pregnant patient in dentistry. J Int Oral Health. 2013; 5(1):88-97.
- Novac L. Producerea placentară de hormoni polipeptidici şi proteici. Producţia placentară de hormoni steroizi. În: Fraga Silvia Paveliu. Endocrinologia gravidei. Ed. InfoMedica, 2003.
- Gheorghiu IM, Mitran M, Mitran L, Pană DP, Mironiuc Cureu M. Gingivita de sarcină. ORL.ro. 2012; 14(1):42-3.
- Soares PV, Machado AC, Zeola LF, Souza PG, Galvão AM, Montes TC, Pereira AG, Reis BR, Coleman TA, Grippo JO. Loading and composite restoration assessment of various non-carious cervical lesions morphologies – 3D finite element analysis. Aust Dent J. 2015; 60(3):309-16.
- Alcantara PM, Barroso NFF, Botelho AM, Douglas-de-Oliveira DW, Gonçalves PF, Flecha OD. Associated factors to cervical dentin hypersensitivity in adults: a transversal study. BMC Oral Health. 2018; 18(1):155.
- Russell SL, Mayberry LJ. Pregnancy and oral health: a review and recommendations to reduce gaps in practice and research. MCN Am J Matern Child Nurs. 2008; 33(1):32-7.
- Lee JM, Shin TJ. Use of local anesthetics for dental treatment during pregnancy; safety for parturient. J Dent Anesth Pain Med. 2017; 17(2):81–90.
- Patil S, Thakur R, K M, Paul ST, Gadicherla P. Oral health coalition: knowledge, attitude, practice behaviours among gynaecologists and dental practitioners. J Int Oral Health. 2013; 5(1):8-15.
- Brown KM, Gillespie G. Advancements in composite resin material enable streamlined direct restoration process. Compend Contin Educ Dent. 2019; 40(suppl 2):2-6.
- Giuliani M, Grossi GB, Pileri M, Lajolo C, Casparrini G. Could local anesthesia while breast-feeding be harmful to infants? J Pediatr Gastroenterol Nutr. 2001; 32(2):142-4.
- Kierklo A. Restorative treatment of cervical tooth lesions in aspect of biomechanics. Wiad Lek. 2008; 61(1-3):53-7.

Dinamica ţesuturilor periodontale în menopauză
Alexandru Iliescu, Paula Perlea, Kamel Earar, Irina-Maria Gheorghiu, Mihaela Georgiana Iliescu, Andrei Iliescu, Loredana Mitran, Mihai Mitran
Oscilaţiile hormonale la femei dirijează de-a lungul vieţii variate modificări gingivale. În menopauză, boala parodontală, ca rezultat al interacţiunii microflorei orale patogene cu ţesuturile loc...
Biomarkeri în endometrioză
Alexandra Bouariu, Corina Gică, George Iancu, Radu Botezatu, Gheorghe Peltecu
Endometrioza reprezintă o boală debilitantă, estimându-se a afecta 10% dintre femeile la vârstă reproductivă. Endometrioza se caracterizează prin implanturi de ţesut endometrial în afara cavităţii uterine. Laparoscop...
Ecografia în endometrioza infiltrativă profundă
Anca Daniela Stănescu, Romina-Marina Sima, Denisa-Oana Bălălău, Alina Talpalaru, Liana Pleș
Introducere. Endometrioza cu diferite grade de severitate afectează aproximativ 5% dintre femei. Aceasta poate implica ovarele, peritoneul pelvian, fundul de sac Douglas (POD), rectul, rectosigmoidul, septul rectovaginal...
Dinamica ţesuturilor periodontale în menopauză
Alexandru Iliescu, Paula Perlea, Kamel Earar, Irina-Maria Gheorghiu, Mihaela Georgiana Iliescu, Andrei Iliescu, Loredana Mitran, Mihai Mitran
Oscilaţiile hormonale la femei dirijează de-a lungul vieţii variate modificări gingivale. În menopauză, boala parodontală, ca rezultat al interacţiunii microflorei orale patogene cu ţesuturile loc...
Restaurarea coronară cu rășini compozite utilizând „stamp technique” – prezentare de caz
Irina-Maria Gheorghiu, Mihai Mitran, Loredana Mitran, Alexandru-Andrei Iliescu
Restaurarea directă a pierderilor de substanță dură dentară apărute ca urmare a leziunilor carioase este realizată la ora actuală cu ajutorul materialelor adezive, între care rășinile compozite ocupă...