Abordarea chirurgicala a unui nodul pulmonar solitar la un pacient cu o neoplazie in antecedente
Surgical approach for a solitary pulmonary nodule in a patient with history of malignancy
Abstract
A solitary pulmonary nodule represents a radiological opacity, of 3 cm diameter or less, surrounded by normal lung parenchyma, with no other abnormalities on the CT scan. The differential diagnosis of solitary pulmonary nodules includes over 100 conditions, lung cancer being the most frequent (53% of nodules <3 cm). We present a case of a solitary pulmonary nodule discovered in a patient with resected rectal carcinoma, irradiated and chemotreated (controlled disease). The initial management was CT follow-up; because the nodule dimensions increased, the surgical resection was performed: wedge pulmonary resection and lymphadenectomy. The pathological diagnosis was stage IA lung adenocarcinoma. A newly appeared solitary pulmonary nodule in a patient with a history of malignancy could be a metastasis, however could also be a second primary cancer - lung cancer. Wedge pulmonary resection and lymphadenectomy is an appropriate surgical management for stage IA lung cancer in selected patients; this approach impose close follow-up for early detection of a local relapse.Keywords
solitary pulmonary nodulepulmonary wedge resectionlymphadenectomystage IA lung cancerRezumat
Un nodul pulmonar solitar reprezintă o opacitate radiologică, mai mică de 3 centimetri, înconjurată de parenechim pulmonar normal, fără alte modificari pe CT (Computer Tomograf). Diagnosticul diferenţial al nodulilor pulmonari solitari include peste 100 de afecţiuni, cancerul pulomonar fiind cea mai frecventă ( 53% din nodulii sub 3 cm). Vă prezentăm un caz cu un nodul pulmonar solitar descoperit la un pacient cunoscut cu un carcinom rectal rezecat, radio- şi chimiotratat. Abordarea iniţială a fost urmărirea CT; deoarece dimensiunile nodulului au crescut, s-a optat pentru intervenţie chirurgicală: rezecţie pulmonară limitată şi limfadenectomie.Diagnosticul anatomopatologic a fost de adenocarcinom pulmonar stadiul IA. Un nodul nou apărut la un pacient cu istoric de neoplazie poate fi o metastază, dar poate fi şi un al doilea cancer - cancer pulmonar. Rezecţia limitată şi limfadenectomia este o metodă viabilă pentru un cancer pulmonar în stadiul IA, la pacienţi selectaţi; această abordare impune reevaluări frecvente pentru detecţia precoce a unei recidive locale.
Cuvinte Cheie
nodul pulmonar solitarrezecţie limitată pulmonarălimfadenectomiecancer pulmonar stadiul IAIntroduction
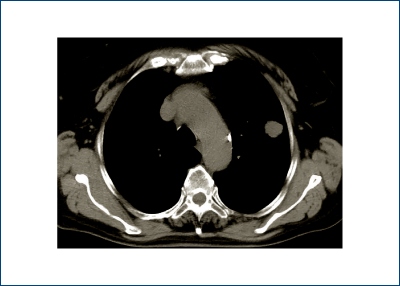
“A solitary pulmonary nodule is a single, spherical, well-circumscribed, radiographic opacity that measures less than or equal to 3 centimeters in maximal diameter and is surrounded completely by aerated lung. There should not be any associated atelectasis, hilar enlargement or pleural effusion” - definition according to Gould and associates and the American College of Chest Physicians (ACCP), evidence-based clinical guidelines for lung nodules(1) - figure 1.
Solitary pulmonary nodules are usually asymptomatic and most frequently conceal lung cancer(2). Cancer risk increases with age, male gender and a smoking history. Malignant lesions are usually represented by lung cancer while granulomas constitute a majority of the benign tumors, hamartomas accounting for the largest proportion of these(3). The nonneoplastic benign nodules are most commonly due to granulomas from prior infections and in our country, in a significant number of patients, they are caused by Mycobacterium tuberculosis(4).
Solitary pulmonary nodules in patients with a history of malignancy other than lung cancer have a higher chance of being metastatic. Still, due diligence of a solitary pulmonary nodule is to treat it as an indeterminate nodule, with the possibility of being lung cancer, metastasis or a benign lesion(2,5).
Materials and methods
We present the case of a 50-year-old female patient, with a known history of rectal epidermoid basaloid carcinoma G2 removed a year ago via abdominoperineal resection of the rectum with clear resection limits, who underwent chemotherapy and radiotherapy and discovers a left pulmonary nodule on the CT scan.
From the patient’s history we mention Parkinson’s disease, medicated major depressive disorder and high risk arterial hypertension - which required drug dose modifications prior to surgery.
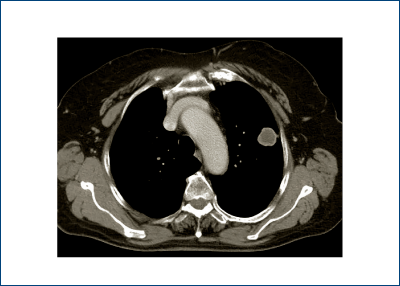
CT scan follow-up of the pulmonary nodule at 6 months revealed growth from 1.6 cm to 2.6 cm, a clear indication for surgical treatment (figure 2).
Results
Following completion of clinical and paraclinical investigations and maintenance of her arterial hypertension we proceeded to surgery, performing a nonanatomic resection of the left superior lobe. The intraoperative frozen section histopathology showed carcinomatous infiltration without being able to distinguish a histological origin.
Considering the patient’s heart conditions, in spite of the possibility of being lung cancer, we limited our procedure to a nonanatomical pulmonary resection and added lymphadenectomy: hilar and mediastinal, prevascular, subaortic, pulmonary ligament and paraesophageal stations (10, 9, 8, 5, 3a).
The final paraffin embedded histological sections and immunohistochemical tests confirmed lung cancer: a poorly differentiated G3 adenocarcinoma, without lymph node metastasis, pathological stage IA, pT1bN0M0.
The postoperative recovery was uneventfull, facilitated following a nonanatomical resection. The patient was forwarded towards the oncology ward. The therapeutical decision was follow-up.
Discussion
The prevalence of solitary pulmonary nodules in the general population is unknown. Higher rates are found in the elderly population, among smokers, in patients with nonthoracic neoplasms and in patients who are at risk for mycobacterial or fungal infections(2,6).
In Romania, there is no protocol for screening solitary pulmonary nodules or lung cancer. Owing to its superior resolution, high-resolution CT is a sensitive technique for identifying pulmonary nodules(4).
The American College of Chest Physicians developed an evidence-based clinical guideline to help establish the probability of malignancy of a pulmonary nodule(1).
Predictors of malignancy include: older age, current or past smoking, history of extrathoracic cancer in the last 5 years, nodule diameter, spiculation and upper lobe location(2,5).
Predictors of a benign nodule are: age under 35, location in an endemic area of granulomatous disease, respiratory symptoms of acute infection, certain patterns of calcifications, stability over time (2 years) and lack of presence of cancer cells in transthoracic needle biopsy(6,7).
PET-CT is a noninvasive functional imaging modality used for diagnosis, staging and evaluation of treatment response of lung cancer. PET-CT is not indicated for nodules that are under 0.7-0.8 cm. In patients at risk for lung cancer and with indeterminate nodules on CT scan, a negative PET-CT does not eliminate malignancy. If it’s a positive PET-CT scan nodule, we can guide the patient to further invasive investigations - transthoracic needle aspiration biopsy or bronchoscopy, depending on the location of the nodule(8,9).
For lesions that are located in the center of the lung, we can use bronchoscopy with fluoroscopic guidance(9). For nodules situated in the outer third of the lung, transthoracic needle biopsy can help obtain a diagnosis. With a higher number of biopsy samples taken and a good on-site cytopathologyst, one may obtain a higher rate of positive results(10).
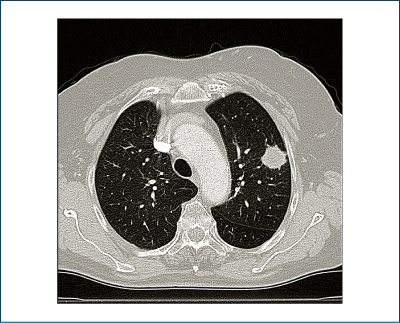
Having a history of extra thoracic cancer, our patient’s solitary nodule has a higher risk of metastasis. However, the imaging characteristics (figures 1, 2, 3) classified it as an indeterminate nodule, and therefore compelled us to also consider lung cancer as a possibility.
Our thoracic surgery clinic in National Institute of Oncology proposed in 2010 a protocol for solitary nodule based on the existence of a CT scan available, regardless of the possibility of invasive diagnostic methods (biopsy by bronchoscopy or transthoracic)(4).
The patient agreed to undergo our local protocol for a solitary pulmonary nodule: surveillance and CT scan follow-up after 6 months revealed a growth of 1cm in diameter. Considering she had multiple predictors of malignancy: growth over time, extra thoracic cancer in the last 5 years, the nodule was in an upper lobe (of the left lung), we decided that the best conduct is surgery.
Wedge pulmonary resection completed with lymphadenectomy was the appropriate surgical procedure considering the patient’s status, granting an easier postoperative period with a shortened recovery time and a better quality of life.
The significant percentage of malignancy in pulmonary nodules justifies aggressive attitude for indeterminate nodules - „surgical resection with curative intention”(4).
Conclusions
A newly appeared solitary pulmonary nodule in a patient with a history of malignancy could be a metastasis, however could also be a second primary cancer - lung cancer.
Wedge pulmonary resection and lymphadenectomy is an appropriate surgical management for stage IA lung cancer in selected patients; this approach imposes close follow-up for early detection of a local relapse.
Bibliografie
1. Gould MK, Fletcher J, Iannettoni MD, Lynch WR, Midthun DE, Naidich DP, Ost DE. American College of Chest Physicians. Evaluation of patients with pulmonary nodules: when is it lung cancer?: ACCP evidence-based clinical practice guidelines (2nd edition). Chest. 2007;132(3 Suppl): 108S-130S.
2. Clements WM, DeRosimo JF, Reed CE. Solitary Pulmonary Nodule. In: Shields, TW, LoCicero J, Reed CE, Feins RH (eds). General Thoracic Surgery, 7th Edition, Ed 2009 Lippincott Williams & Wilkins 2009, 1205-1211.
3. Shileds TW. Pathology of Carcinoma of the Lung. In: Shields, TW, LoCicero J, Reed CE, Feins RH (eds). General Thoracic Surgery, 7th Edition, Ed 2009 Lippincott Williams & Wilkins 2009, 1311-1340.
4. Motaş N, Motaş C, Davidescu M, Bluoss C, Rus O, Bobocea A, Vasilescu F, Horvat T. Nodulul pulmonar solitar - 150 cazuri operate. Chirurgia, 2010 (2): 195-201.
5. Horvat T, Nicodin A, Motaş C. Cancerul bronhopulmonar. In: Popescu I, ed. Tratat de Chirurgie, Horvat T ed, Vol.IV : Chirurgie Toracică. Ed Academiei Române, Bucureşti 2008; 569-618.
6. Horvat T, Nicodin A. Tratamentul chirurgical in cancerul bronhopulmonar. In: Cancerul bronhopulmonar. Horvat T, Dediu M, Ţârlea A (eds). Editura Universul, Bucuresti, 2000;209-259.
7. Shrager JB, Cooper JD. Investigation and management of the indeterminate pulmonary nodule. In: Pearson’s Thoracic and Esophageal Surgery. Patterson GA, Pearson FG, Cooper J, Deslauriers J, Rice T, Lucketich J, Lerut A (eds). 3rd ed. Ed. Churchill-Livingstone, London, 2008: 455-461.
8. Fultz PJ, Feins RH. Radiologic Evaluation of Lung Cancer. In: Shields, TW, LoCicero J, Reed CE, Feins RH (eds). General Thoracic Surgery, 7th Edition, Ed 2009 Lippincott Williams & Wilkins 2009, 1361- 1374.
9. Gould MK, Maclean CC, Kuschner WG, Rydzak CE, Owens DK. Accuracy of positron emission tomography for diagnosis of pulmonary nodules and mass lesions: a meta-analysis. JAMA. 2001; 285(7):914-24. Comment in: ACP J Club. 2001; 135(2):73. JAMA. 2001; 285(7):936-7.
10. Anocha S, Sharma S, Maycher B. Solitary pulmonary nodule. At http://emedicine.medscape.com/article/36 2787- overview. Updated: Apr 30, 2009, accessed at Nov 17, 2009.

Tumorile neuroendocrine - diagnostic şi strategii terapeutice
Ioana Luca
NETs are rare diseases. There is a lack of robust source data on epidemiology Nothing exists to describe the overall European situation: Only individual country data exists ENETS in process of establishing a pan-European registry. Rare locations: Liver and biliary system (0.59%) Gall bladder (0.31...
Cancerul şi obezitatea - implicaţii etiopatogenice, clinico-evolutive şi terapeutice
Ciprian Cirimbei, Elena Chitoran, Oana Păvăleanu, V. Rotaru, D. Straja
Obezitatea constituie un factor cu impact major în dezvoltarea unor cancere genitale şi digestive, cu mecanisme etiopatogenice parţial elucidate, dar implică totodată şi o diagnoză uneori mai dificilă, precum şi un parcu...
Cancerul, o problemă nerezolvată
Doru Paul
Pornind de la ideea că eşecul nostru de a vindeca cancerul vine din lipsa noastră de a înţelege complexitatea sa, ştiinţa contemporană priveşte trei modele principale pentru înţelegerea cancerului: 1. xenobiontul, 2. simbiontul, 3. oncobiontul. Fiecare prototip va fi detaliat cu suişuri, aşteptări şi nereuş...
Metastaze skip şi supravieţuirea - argumente pentru disecţia ganglionilor limfatici în cancerul pulmonar
Natalia Motaş, Robert Nicolae, Elena Moise, Teodor Horvat
Lung cancer continues to be the most common cause of death related to cancer per year and the number is increasing every year. One case out of 10 is resectable, with chances of cure. Lymphatic spread ...
Giant solitary lung metastasis from an osteosarcoma (malignant fibrous histiocytoma-like) of the spine
Alin Burlacu, Flavia Ultimescu, Aurelia Alexandru, B. Tănase, Laurenţia Galeş, M. Mugescu, Violeta Deaconescu, Teodor Horvat
Prezentăm cazul unui bărbat nefumător, în vârstă de 69 de ani, care a venit la spital pentru dispnee, dureri toracice, hemoptiz...