Diagnostic challenges in recurrent respiratory infections in children – the vascular ring. A case report
Dificultăţi de diagnostic în infecţiile respiratorii recurente la copil – inelul vascular. Prezentare de caz
Abstract
Introduction. Recurrent respiratory infections in the pediatric population are among the most frequent reasons for requesting medical care. The physician must have a clear judgment to establish the diagnosis, as the causes are very heterogeneous. A thorough evaluation of the family history, environmental exposures and allergies are the key elements in the diagnostic process. A rare cause of recurrent respiratory tract infections is the vascular ring, resulting in the compression of the trachea and/or the esophagus, causing respiratory and/or digestive symptoms. It is often misdiagnosed due to its rarity, and the proper treatment is delayed. Case report. We present the case of a 7-month-old infant who was transferred to our gastroenterology department to treat an invasive Campylobacter jejuni infection, which rapidly evolved well. However, during her hospital stay, we learned that our patient had a significant history of recurrent respiratory infections of medium severity, leading us to investigate further a possible immunodeficiency, either primary or secondary. The clinical exam showed no relevant anomalies, but laboratory studies revealed a deficit in immunoglobulins A and M and a low CD4/CD8 T-cell ratio. Initially, the case was interpreted as a primary humoral immunodeficiency; however, the immunoglobulin levels later normalized. Chest X-ray showed an extrinsic compression of the trachea and the absence of the aortic knob. Bronchoscopy confirmed the narrowing of the tracheal lumen and thoracic CT angiogram revealed the presence of an aortic arch anomaly, namely a right aortic arch with an aberrant left carotid artery. Therefore, the diagnosis of vascular ring was established. Conclusions. Recurrent respiratory infections in children can be a diagnostic challenge. Anamnesis, clinical exam, laboratory and imaging data must be logically structured to have a clear insight into the case. Otherwise, crucial details can be omitted, and the correct diagnosis cannot be established. Although vascular rings are rare, they should not be overseen when the more common causes of frequent respiratory infections have been excluded.Keywords
recurrent infectionsimmunodeficiencypassive smokingtracheal compressionvascular ringRezumat
Introducere. Infecţiile respiratorii recurente sunt cauze frecvente de solicitare a consultului medical în populaţia pediatrică. Cauzele acestor manifestări sunt foarte variate, astfel încât o încadrare corectă necesită o judecată clinică atentă. În acest context, anamneza detaliată a antecedentelor heredocolaterale, a expunerii la toxice şi a posibilelor alergii devine indispensabilă stabilirii corecte şi precoce a diagnosticului. O etiologie rară a infecţiilor respiratorii repetate este reprezentată de inelul vascular, care determină compresiunea structurilor învecinate – şi anume, a traheii şi esofagului. Consecinţa este apariţia simptomelor respiratorii şi digestive, cu răsunet variabil. Această anomalie congenitală vasculară este frecvent subdiagnosticată şi, drept urmare, se întârzie în instituirea tratamentului. Prezentarea cazului. Prezentăm cazul unui sugar de sex feminin, în vârstă de 7 luni, care a fost transferat în serviciul de gastroenterologie pediatrică, în contextul unei infecţii invazive cu Campylobacter jejuni. Evoluţia infecţiei a fost favorabilă, însă la reluarea anamnezei am identificat în antecedentele personale ale pacientei multiple infecţii, în principal respiratorii, de severitate medie. În acest context, am efectuat investigaţii pentru evaluarea unei eventuale imunodeficienţe, fie primară, fie secundară. Examenul clinic nu a evidenţiat aspecte semnificative, însă paraclinic s-au decelat un deficit imun umoral de IgA şi IgM şi anomalii nespecifice ale imunităţii celulare (raport CD4:CD8 scăzut). Cu toate acestea, diagnosticul de deficit imun primar nu a putut fi stabilit, deoarece la scurt timp valorile imunoglobulinelor serice s-au normalizat spontan. Am efectuat o radiografie toracică, pe care s-a pus în evidenţă o compresiune extrinsecă a traheii, asociată cu absenţa butonului aortic la nivelul arcului superior stâng. Bronhoscopia a confirmat îngustarea traheii, iar examinarea CT cu substanţă de contrast a toracelui a identificat o anomalie vasculară la nivelul arcului aortic – şi anume, un inel vascular prin arc aortic drept cu traiect aberant al arterei subclavii stângi. Concluzii. Infecţiile respiratorii recurente pot reprezenta frecvent o provocare diagnostică. Datele anamnestice, ale examenului obiectiv, parametrii de laborator şi detaliile imagistice trebuie structurate logic, pentru a dobândi o imagine clară a cazului. În caz contrar, stabilirea diagnosticului corect va fi puţin probabilă. Deşi inelul vascular este o patologie rară, acesta nu trebuie omis atunci când alte diagnostice, cu frecvenţă mai mare la nivelul populaţiei, au fost infirmate.Cuvinte Cheie
infecţii recurenteimunodeficienţăfumat pasivcompresiune trahealăinel vascularIntroduction
Recurrent respiratory infections in the pediatric population are among the most frequent reasons for requesting medical care(1). The most accurate definition of recurrent infections includes frequency, severity and duration criteria(2). The physician needs to have a clear judgment to classify them, as the causes are very heterogenous, from the common gastroesophageal reflux to potentially life-threatening pathologies, such as immune deficiencies(3). The differential diagnosis is broad and, therefore, when examining such a patient, it is essential to consider all possibilities. As it is the case for every symptom in a child, to direct oneself towards the correct spectrum of diseases, one should consider the patient’s age. Moreover, multiple etiologies can overlap, thus making a thorough evaluation of family history, environmental exposures and allergies a key element in the diagnostic process. This is of even greater importance when an apparently logical, more plausible cause of the infections may arise(2).
A rare cause of recurrent respiratory tract infections is the vascular ring, a congenital anomaly of the aortic arch. If the ring completely encircles the adjacent structures, it compresses the trachea and/or the esophagus and results in respiratory and digestive manifestations(4). It is often misdiagnosed and the proper treatment is delayed due to its rarity, making such a case a real challenge(5).
Case report
We present the case of a 7-month-old infant transferred to our pediatric gastroenterology department for the proper treatment of an invasive Campylobacter jejuni infection. She had been hospitalized in another clinic for acute bronchiolitis with associated acute respiratory failure that had remitted. However, the patient developed a persisting diarrheic syndrome and fever. The clinical findings were correlated with laboratory studies that showed an important inflammatory syndrome, with elevated C-reactive protein level (CRP 7.04 mg/dl) and procalcitonin level (75.62 ng/ml). Specific antibiotic therapy was started at that moment, and the patient was transferred to our medical ward.
During her hospital stay, we learned that our patient had a significant history of recurrent respiratory infections of medium severity, leading us to investigate further a possible immunodeficiency, either primary or secondary. Clinically, we noticed a well-nourished girl with a doll-like face. She had no skin lesions or superficial lymph nodes and tonsils were present and of normal dimensions. She presented abundant mucopurulent rhinorrhea, a hyperemic pharynx, dysphonia, stridor triggered by crying and a spastic cough, with no rales on lung auscultation. Cardiovascular system evaluation revealed a systolic heart murmur, best heard at the left sternal border. She did not take any chronic medication. The complete blood count showed nonspecific alterations, such as monocytosis, and neutrophil, lymphocyte and thrombocytes count levels were normal. Two quantitative pilocarpine iontophoresis sweat tests were conducted, and both were negative. Serum immunoglobulins were in the normal range. Quantitative lymphocyte subsets were ordered and revealed a low CD4/CD8 ratio of no apparent significance, as CD4 lymphocytes and CD8 lymphocytes were of a normal absolute value. In the setting of a clinically discernable heart murmur, echocardiography was done; it revealed the presence of multiple anomalies: a patent ductus arteriosus, a patent foramen ovale and a weakly visualized aortic arch. Regarding the digestive infection, the evolution was good; diarrhea and fever remitted completely and inflammatory parameters returned to normal values.
Subsequent follow-ups exposed a possible explanation of our patient’s recurring infections. A humoral immune deficit appeared to develop, consisting of an immunoglobulin A deficit that later associated an immunoglobulin M lower level. IgE levels were slightly elevated. Human immunodeficiency virus (HIV) serology was negative for the mother and the patient.
During two months, the patient had five presentations for mucous rhinorrhea, productive cough and dyspnea, intermittently associated with fever, dysphonia and stridor. We discussed the living conditions our patient was exposed to in greater detail with the mother. She is the second child of the family and lived in a deprived neighborhood of the city. Their home consisted of one room, which sheltered two adults, two children and one dog. Moreover, the parents admitted they were both smoking inside the house in the presence of the infant.
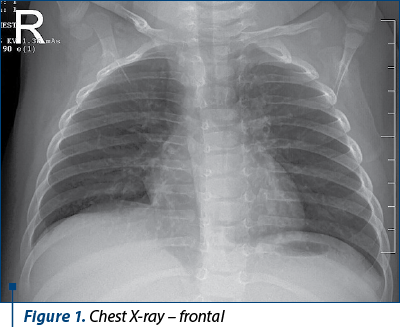
During a respiratory infection episode, we performed a chest X-ray that revealed bilateral lung hyperinflation and a narrowing of the second third of the trachea, on the right side, that seemed to be extrinsic (Figure 1). Moreover, the left cardiomediastinal contour lacked the aortic knob. A bronchoscopy was safely performed, and it confirmed the extrinsic compression of the trachea.
Firstly, primary tuberculosis had to be excluded, as mediastinal lymph node enlargement could be responsible for the radiological changes. Bronchoalveolar lavage fluid was collected for Ziehl-Neelsen smear and Loewenstein-Jensen medium culture. Blood samples for Quantiferon-TB Gold were also taken. All results came out negative.
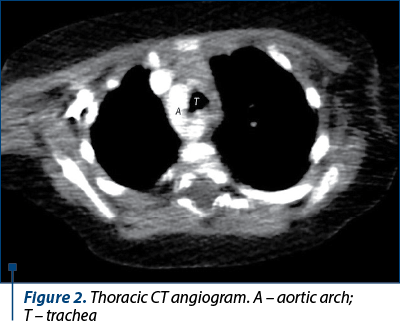
To identify the structure that caused partial tracheal obstruction, a computed tomography (CT) angiogram was ordered. It described a right aortic arch (Figure 2) with an aberrant left subclavian artery and the right subclavian and common carotid arteries with independent origins from the aortic arch.
In the meantime, we evaluated the infant in the absence of an acute infectious disease. Laboratory studies showed normal values of serum immunoglobulins, proving that the immune deficit was probably transitory.
Discussion
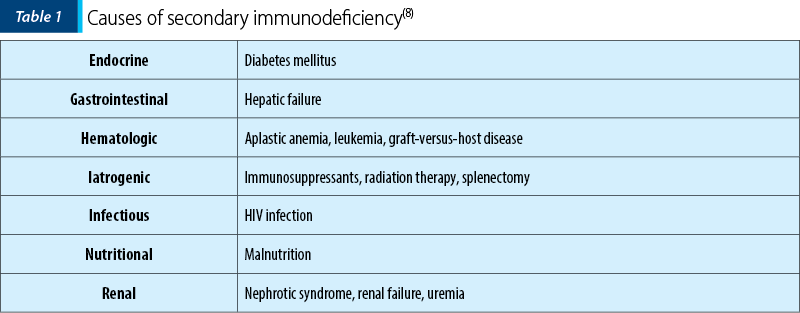
Establishing the correct diagnosis in a child with recurrent infections can be challenging. The differentiation between common causes of infection in early childhood and potentially life-threatening immune deficiencies or other rare causes is imperative, as early diagnosis and specific treatment improve the quality of life in these patients. It is well-known that normal children develop multiple infections, especially during the early years, but an increase in number, duration and severity can indicate an underlying problem(6). Immunodeficiencies can be primary or secondary, the latter being more frequent and with a large variety of causes, noted in Table 1(7). Even atopy is a risk factor for frequent respiratory infections, the mechanism being related to the chronic inflammation of the mucosa, leading to increased pathogen adherence(2).
Our patient’s clinical and laboratory studies did not indicate any of the enumerated causes. She was well-nourished, blood glucose and the glycemic profile were normal. The parents did not describe any allergic manifestations and she did not take any immunosuppressive agents. Liver and kidney function were normal, and no malignancy or chronic infection were found. Considering these facts and that she subsequently developed low levels of immunoglobulins, a primary immunodeficiency was more probable. This was even more plausible, as IgA and IgM levels were persistently low on multiple occasions. However, these laboratory studies were conducted during an ongoing acute respiratory infection, as we could not record any disease-free interval at first.
A major risk factor for respiratory infections in our patient was second-hand smoking. Multiple studies have demonstrated the link between child cigarette smoke exposure and respiratory symptoms, such as cough, wheeze and abundant phlegm production. The risk is significantly higher if both parents smoke(9). The mechanism by which the respiratory tract is more prone to infection, even in passive smokers, is that cigarette smoke increases mucus secretion and decreases cilia motility(10). Moreover, second-hand smoking is proven to cause a slight elevation in IgE levels, which is the case in our patient, even though she had not developed any allergic manifestations. These high IgE levels might be associated with respiratory tract sensitization, indicating that exposed children might develop asthma later(9). Cigarette smoke causes more profound immune dysregulations, as two experimental studies have proven. CD4:CD8 T-cell ratio appears to be modified by smoke exposure, with a dominance of CD8 T-lymphocytes. Although nonspecific, this finding of a low CD4:CD8 ratio in our patient seems to be associated with environmental exposure to cigarette smoke. Interestingly, it is cited that the ratio normalizes at about six weeks after exposure cessation. However, we have not repeated quantitative lymphocyte subsets(11,12).
In an extrinsic tracheal obstruction setting, the cause must be identified to proceed with the proper treatment. We narrowed the differential diagnosis to two possibilities: a mediastinal lymph node or a vascular ring. Lymphadenopathies localized in the mediastinum are typical for primary tuberculosis; given that the patient pertains to a low-income environment and that tuberculosis rates are still relatively high in our country, we considered this supposition to be pertinent(13). As the patient had received the BCG vaccine soon after birth and all specific diagnostic tests were negative, we excluded the possibility of Mycobacterium tuberculosis primoinfection.
Vascular rings are congenital aortic arch anomalies that can compress the tracheobronchial tree, being a rare cause of recurrent respiratory symptoms in children. It can manifest variably, most often by stridor, frequent respiratory infections, cough and wheezing(4). Medical literature has reported the case of a 19-year-old young woman that was similar to ours. Since early infancy, she started developing recurrent pneumonia and upper respiratory tract infections that were not alleviated by any treatment. She received inhaled corticosteroids, multiple antibiotic courses, specific medication for gastroesophageal reflux disease and allergic rhinitis, with no reduction in infection frequency whatsoever. Spirometry suggested a central airway obstruction, leading the medical team to perform bronchoscopy and a thoracic CT, finally establishing the vascular ring diagnosis. Surgical correction was conducted, and all symptoms were remitted after that(5).
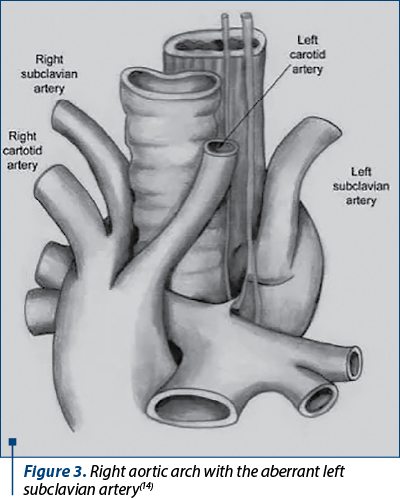
There are different anatomical variations to the vascular ring. Two of them are the most common: the double aortic arch (30-45% of cases) and the right aortic arch with the aberrant left subclavian artery (30-60% of cases). In our case, the latter was present. The ring was complete and composed of the following structures: the aortic arch anteriorly and to the right, the origin of the subclavian artery posteriorly, and the ductus arteriosus to the left (Figure 3). It is typical for this malformation that the left common carotid artery emerges from the aortic arch. The right common carotid artery and right subclavian artery have separate origins from the arch, the brachiocephalic trunk being absent. The explanation for these anomalies lies in the embryological development of the six pairs of aortic arches, but this is not the main subject of the current paper. Hence, it will not be discussed in greater detail(15). An important aspect of vascular rings is that they are frequently associated with other malformations. Reports suggest that 50% of children with this diagnosis also present other congenital anomalies; both cardiac and noncardiac, patent ductus arteriosus, ventricular sept defects, tracheoesophageal fistulas and cleft lip-palate are mentioned(4). Our patient confirmed this theory, as patent ductus arteriosus was identified, emphasizing the importance of cardiac ultrasound when tackling such a case.
In symptomatic cases, the treatment options are limited to surgery, as mechanical compression cannot be relieved using medication. It consists of the surgical division of the ring, in this case, the ductus arteriosus being the sectioning site. The results are encouraging, as most children present postoperative symptom relief during the first year(4,16). Regarding our patient, the surgery was scheduled soon.
Conclusions
Recurrent infections are among the most frequent yet potentially difficult medical encounters in pediatrics, as the diagnostic possibilities are vast. Anamnesis, clinical exam, laboratory and imaging data must be logically structured to obtain a clear insight into the case. Otherwise, crucial details can be omitted, and the correct diagnosis cannot be established. Although congenital arterial anomalies, such as vascular rings, are rare, they should not be overseen when the more common causes of frequent respiratory infections have been excluded. Another important aspect highlighted by this case is the importance of environmental factors, such as passive smoking, regarding the respiratory symptoms in infants.
Conflict of interests: The authors declare no conflict of interests.
Bibliografie
-
Jesenak M, Ciljakova M, Rennerova Z, Babusikova E, Banovcin P. Recurrent Respiratory Infections in Children – Definition, Diagnostic Approach, Treatment and Prevention. InTech [Internet]. London: IntechOpen; 2011 [cited 2022 Feb 20]. Available from: https://www.intechopen.com/chapters/17357 doi: 10.5772/19422
-
Butte MJ, Stiehm ER. Approach to the child with recurrent infections. UpToDate; 2020 [updated Dec 29 2020, cited Feb 22 2022]. Available from: https://www.uptodate.com/contents/approach-to-the-child-with-recurrent-infections
-
El-Azami-El-Idrissi M, Lakhdar-Idrissi M, Chaouki S, Atmani S, Bouharrou A, Hida M. Pediatric recurrent respiratory tract infections: when and how to explore the immune system? (About 53 cases). Pan Afr Med J. 2016;24:53. doi:10.11604/pamj.2016.24.53.3481
-
Fulton DR, Prosnitz AR. Vascular rings and slings. UpToDate; 2019 [updated Feb 06 2019, cited Feb 22 2022]. Available from: https://www.uptodate.com/contents/vascular-rings-and-slings
-
Calabrese C, Corcione N, Di Spirito V, Guarino C, Rossi G, Domenico Gargiulo G, et al. Recurrent respiratory infections caused by a double aortic arch: The diagnostic role of spirometry. Respir Med Case Rep. 2013;8:47-50. doi:10.1016/j.rmcr.2012.12.006.
-
Alkhater SA. Approach to the child with recurrent infections. J Family Community Med. 2009;16(3):77-82.
-
Ress S. Investigation of adult immunodeficiency and indications for immunoglobulin replacement therapy. S Afr Med J. 2014;104(11):791-792.
-
Neskovic V. Preoperative assessment of the immunocompromised patient. Acta Chir. 2011;58:185-92.
-
Samet JM, Sockrider M. Secondhand smoke exposure: Effects in children. UpToDate; 2021 [updated Feb 23 2021, cited Mar 1 2022]. Available from: https://www.uptodate.com/contents/secondhand-smoke-exposure-effects-in-children.
-
Liu Y, Di YP. Effects of second hand smoke on airway secretion and mucociliary clearance. Front Physiol. 2012;3:342. doi: 10.3389/fphys.2012.00342.
-
Motz GT, Eppert BL, Sun G, Wesselkamper SC, Linke MJ, Deka R, et al. Persistence of Lung CD8 T Cell Oligoclonal Expansions upon Smoking Cessation in a Mouse Model of Cigarette Smoke-Induced Emphysema. J Immunol. 2008; 181(11):8036-8043. doi: 10.4049/jimmunol.181.11.8036
-
Fusby JS, Kassmeier MD, Palmer VL, Perry GA, Anderson DK, Hackfort BT. Cigarette smoke-induced effects on bone marrow B-cell subsets and CD4+:CD8+ T-cell ratios are reversed by smoking cessation: Influence of bone mass on immune cell response to and recovery from smoke exposure. Inhal Toxicol. 2010;22(9):785-796.
-
Golli AL, Niţu MF, Turcu F, Popescu M, Ciobanu-Mitrache L, Olteanu M. Tuberculosis remains a public health problem in Romania. Int J Tuberc Lung Dis. 2019;23(2):226-231. doi: 10.5588/ijtld.18.0270.
-
Bhimji S. Vascular Rings. Medscape Drugs & Diseases. 2021 Apr 22; Cited 2022 Mar 1. Available from https://emedicine.medscape.com/article/426233-overview.
-
Hanneman K, Newman B, Chan F. Congenital Variants and Anomalies of the Aortic Arch. RadioGraphics. 2017; 37:32–51.
-
Amir G, Soffair N, Frenkel G, Bruckheimer E, Nachum E, Rotshtein A, et al. Vascular ring surgery – can we do better? Eur Heart J. 2020;41(2):3210.

Acute liver failure associated with recent SARS-CoV-2 infection in a pediatric patient – case report
Georgiana Laura Cioancă, Alina Grama, Luciana Petrescu, Simona Căinap, Bianca Raluca Mateescu, Gabriel Benţa, Bogdan Bulata, Tudor Lucian Pop
Insuficienţa hepatică acută (IHA) la copil este o patologie rară, dar severă, caracterizată prin coagulopatie şi modificări de lab...
Consequences of anemia in pregnancy upon the newborn – a cross-sectional study
Oana-Liliana Atomei, Paula-Paraschiva Monor, Bogdan A. Stana
Anemia la gravide este încă o problemă importantă de sănătate publică. Consecinţele asupra nou-născutului, imediate sau tardive, pot varia de la patologii uşoare la boli severe. Obiectivul principal al studiului...
Sleep-related breathing disorders in the pediatric patient with Prader-Willi syndrome
Sorina Chindriş, Gabriela Vlad, Ana Maria Daviţoiu, Eugenia Buzoianu, Mirela Iancu, Iulia Ţincu, Ioana Adriana Ghiorghiu, Monica Albert, Andrei Zamfirescu, Doina Anca Pleşca
Sindromul Prader-Willi (PWS) este o boală genetică rară, întâlnită cu o incidenţă de 1:15000 de nou-născuţi, identificată la to...
Acute liver failure associated with recent SARS-CoV-2 infection in a pediatric patient – case report
Georgiana Laura Cioancă, Alina Grama, Luciana Petrescu, Simona Căinap, Bianca Raluca Mateescu, Gabriel Benţa, Bogdan Bulata, Tudor Lucian Pop
Insuficienţa hepatică acută (IHA) la copil este o patologie rară, dar severă, caracterizată prin coagulopatie şi modificări de lab...
Portal cavernoma in children – complications and evolution
Diana-Alexandra Borcău, Alina Grama, Simona Căinap, Claudia Simu, Patricia Lorinţiu, Gabriel Benţa, Bianca Raluca Mateescu, Mihaela Coşarcă, Tudor Lucian Pop
Tromboza de venă portă este o afecţiune rară, dar reprezintă o cauză importantă de hipertensiune portală în patologia pediatrică. ...