Provocări în pandemie: pneumotoraxul la copil
Pneumothorax in children – pandemic challenges
Abstract
The COVID-19 pandemic that we are still going through continues to bring challenges in the management of many chronic diseases that change their evolutionary course or is the source of pathologies for which not enough information has yet been accumulated for a common diagnostic and therapeutic denominator, in adults and especially in children. Although most children who had SARS-CoV-2 infection had mild to moderate manifestations, there were also cases with severe forms that frequently associated a chronic pathology with little or no therapeutic control. The authors present the case of a patient diagnosed with noncompliant therapeutic asthma, who after a SARS-CoV-2 infection presented spontaneous pneumothorax, a life-threatening complication that required emergency surgery.Keywords
asthmapneumothoraxCOVID-19Rezumat
Pandemia de COVID-19 cu care încă ne confruntăm continuă să aducă noi provocări în gestionarea multor boli cronice care îşi modifică evoluţia. Pentru multe dintre aceste noi aspecte evolutive nu sunt suficiente informaţii şi nu există încă experienţe clinice şi terapeutice, nici la adulţi, dar nici la copii. Deşi majoritatea copiilor cu infecţie cu SARS-CoV-2 au avut manifestări uşoare până la moderate, au existat de asemenea cazuri cu forme severe care s-au asociat frecvent cu patologii cronice. Autorii prezintă cazul unui pacient diagnosticat cu astm bronşic, necompliant la tratament, care după infecţia cu SARS-CoV-2 a prezentat un pneumotorax spontan. Această complicaţie ameninţătoare de viaţă a necesitat intervenţie chirurgicală de urgenţă.Cuvinte Cheie
astmpneumotoraxCOVID-19Introduction
In March 2020, the World Health Organization (WHO) declared COVID-19 a global pandemic, an unprecedented event for all mankind. At that time, limited data on the new member of the Coronavirus family led us to believe that patients with asthma, as with all chronic lung diseases, had a risk factor for severe disease and increased mortality(1,2).
Currently, it is considered that the morbidity due to SARS-CoV-2 infection in asthmatic patients is different depending on the age group, being lower in children compared to adults. This is probably due to the mechanism used by the virus to invades human cells. Coronaviruses use a spike (S) protein that binds the angiotensin converting enzyme (ACE) 2 receptor, facilitating its viral attachment to the host cell membranes, inducing a multisystemic inflammatory process, including in the lungs, brain and heart.
Although the information is still limited on the impact of COVID-19 infection on asthma and vice versa, studies performed on children reveled that there are three possible mechanisms that reduce the severity of the disease and the rate of complications in children compared to adults. This different behavior is supported by hypereosinophilia and the Th2-type immune response that is associated with a decrease in ACE2 receptors in the nasal mucosa and pneumocytes and also due to the use of corticosteroid therapy in the background treatment that determines the decrease of the number of cells containing ACE2 and TMPRSS2 receptors(3-5).
However, there are also rare cases of severe COVID-19 infection in children with asthma as a comorbidity. The authors present the evolutionary particularities and the management difficulties in the case of a child diagnosed with asthma, partially controlled, with a history of COVID-19 pneumonia, who had distant spontaneous pneumothorax without having associated mechanical ventilation in the past.
Case presentation
We present the case of an 11-year-old child who presented to the emergency reception unit for mixed dyspnea with acute onset, accompanied by polypnea and inefficient dry cough, without fever, RF=40 breaths/min and SpO2=92%.
The patient declared a family history of atopy and SARS-CoV-2 infection (in December 2020), being known to have mild persistent asthma since February 2021, with background treatment with Singulair®, Flixotide® and Ventolin® (when needed), having multiple presentations in the emergency room for asthma exacerbations frequently in an infectious context (H=140 cm, W=23 kg, BMI=11.7 kg/m2).
In May 2021, he was evaluated in the emergency reception unit for severe respiratory dysfunction with oxygen dependence (SpO2=84%) and polypnea (RF=45 breaths/min), the clinical examination objectifying limited coastal excursions, extremities and perioronasal cyanosis, hippocratic fingers, thoracic hypersonicity, stethacoustic having a bilateral pleural “squeak” in the upper third of the thorax, with dry, rare, ineffective cough. Biologically, there was only a slight inflammatory syndrome (CRP=8 mg/l) and leukocytosis with neutrophilia (WBC=17.47/mm3, NEUT=13.96/mm3). The radiological examination of the thorax at admission objectified right pneumothorax (located apically on the right side, with a thickness of 15 mm), enlarged superior mediastinum and a pleural liquid collection, located apically on the left side, with 10 mm thickness. The thoracic CT examination confirmed the aforementioned lesions, to which was added bilateral pleurisy in small quantities, as well as encysted pleurisy at the level of the both large oblique fissures. The imagistic monitoring during evolution objectified basal lung areas with “matte- glass” aspect in the medium third of the left hemithorax, having a bilateral infiltrative appearance, predominantly on the right side (X-ray; Figure 1).

This has raised the suspicion of “long COVID-19”. The evolution was favorable under antibiotic treatment (piperacillin/tazobactam and trimethoprim/sulfamethoxazole), symptomatic and short-term corticosteroid therapy, without considering a surgical treatment for pneumothorax (being minimal and without pulmonary compressive effect). After discharge, the patient did not continue the background therapy of asthma.
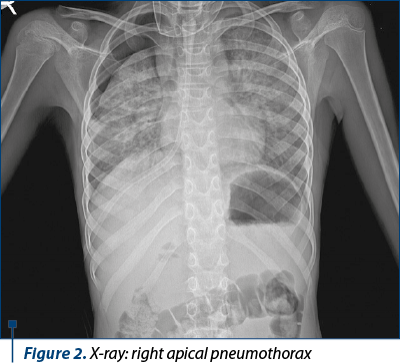
One week after discharge, the respiratory symptoms recurred and the patient was addressed to the regional emergency department, where the degradation of lung lesions was objectified imagistically: right apical pneumothorax with increased thickness, maximum 26 mm, and decreased bilateral pulmonary transparency (X-ray; Figure 2).
Clinically, he developed severe acute respiratory failure symptoms and secondary hypoxia, which is why he was transferred to the pediatric surgery service. Emergency minimal pleurostomy and under water sealed drainage with a 14Ch catheter were performed. The radiographic control objectified right apical compressive pneumothorax having approximately 6 cm, with the presence of the pleural drainage tube in the third right intercostal space (X-ray; Figure 3).

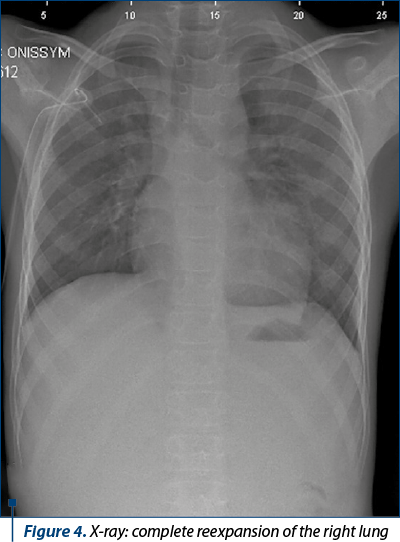
The evolution was slowly favorable, with the remission of the pneumothorax and the complete reexpansion of the right lung (X-ray; Figure 4).
Furthermore, after discharge, the patient did not perform the recommended antiasthmatic background treatment.
The patient returned after two weeks, in the 2nd Pediatrics Clinic, through the emergency department, with a new respiratory recurrence. Clinically, the patient was without fever, but with an affected general condition, with weight loss and mixed dyspnea with polypnea, associated with intercostal and suprasternal circulation, thoraco-abdominal balance, with dry, rare, ineffective cough, and watch-glass nails (Figures 5 and 6).

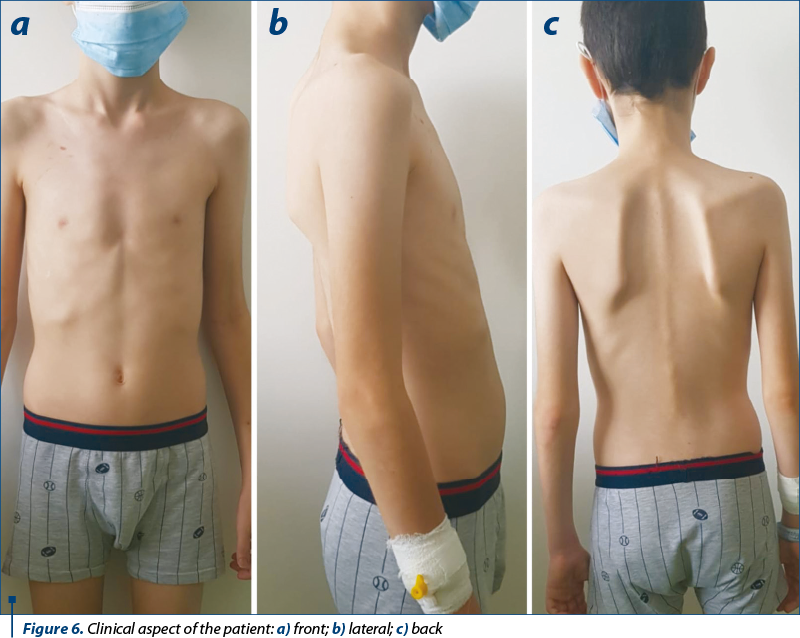
Pulmonary crepitant and subcrepitant rales were objectified, predominantly on the right side.
Biologically, leukocytosis was noted (16460 WBC/mm3) with neutrophilia, and absent COVID-19 antibodies (IgM), IgG=0.96S/CO, allergic polysensitization (specific IgE – increased value) on aeroallergens (pollen, Dermatophagoides pteronyssinus, epithelia and animal veneers), mild toxic-drug hepatocytolysis (four times above normal values). The serology for HVB, HVC, Toxoplasma IgG, IgM, CMV, EBV IgM, and HIV 1 and 2 was negative, but positive for chronic infection with CMV and EBV. Iontophoresis infirmed a possible cystic fibrosis. Quantiferon test, alfa-1 antitrypsin, immunogram – normal values. The chest X-ray objectified a left suprahilar nodular opacity of average intensity of 15/16 mm associated with minimal pleural reaction on the horizontal fissure (possible encysted pleurisy) (X-ray; Figure 7).

The positive diagnosis was: persistent moderate asthma partially controlled with severe exacerbations; intrafamilal SARS-CoV-2 infection; operated right spontaneous secondary pneumothorax; pneumonia with parapneumonic pleurisy; moderate acute respiratory failure; allergic polysensitization; weight hypotrophy (BMI=11.7 kg/m2).
The evolution was favorable under antibiotic therapy, symptomatic and oxygen therapy. Background therapy: Symbicort® 1 puff x 2/day, 6 months, montelukast Na, antihistaminic therapy.
Discussion
There is still little information on the risk factors in SARS-CoV-2 infection in children, especially in those with chronic lung damage, most studies being in adults, which are more frequently symptomatic. But although the pediatric population diagnosed with asthma has a poor innate antiviral immune response and a vulnerability to acute exacerbations due to viral infections, there is evidence of a low susceptibility to SARS-CoV-2 infection(6). Few studies to date support the fact that in children the symptoms are milder in SARS-CoV-2 infection compared to adults, affecting those under 18 years old in approximately 2% of the infections(7).
Although asthma is the most common chronic respiratory disease in children, the current data are insufficient to fully establish whether it is an independent risk factor for SARS-CoV-2 infection or for the severity of its manifestations in the pediatric population. A 2020 CDC report that looked at preexisting conditions in the pediatric population associated with COVID-19 infection revealed that the most common underlying pathologies were chronic lung disease, including asthma(7,8).
Although COVID-19 is less severe in children than in adults, the cases of asthma associated with SARS-CoV-2 infection increase the need for care in a medical setting. Moller et al. argue this in a report in which 61% of patients needed medical care in a pediatric clinic, including the intensive care unit, where 39% of cases required oxygen therapy and 8% required mechanical ventilation. Among these cases treated in the intensive care unit, there was the case of an adolescent with a history of partially controlled asthma, whose evolution was complicated by acute pneumothorax(9).
Spontaneous pneumothorax is a less common entity in children, but one of the most common chest diseases in adolescents, because their mediastinum does not have the fibrous sheath found in adults, which has a role in hindering the air migration. Spontaneous pneumothorax occurs due to increased alveolar pressure such as the cough episode and increased pressure gradient by obstruction of the airways by bronchial hypersecretion, as in the case of asthma. Although, most often, pneumothorax occurs at rest, there are rarer cases in which it occurs after a coughing effort and is associated with asthma, such as in the case of our patient(10).
Due to structural lung damage caused by viral infection, even in the absence of mechanical ventilation, spontaneous pneumothorax may occur as a sequela of COVID-19 pneumonia. In our case, the family history of COVID-19 and the absence of mechanical ventilation strengthens the suspicion that SARS-CoV-2 infection could have been the cause of pneumothorax in this patient(11-13).
Although asthmatic patients have a higher risk of developing spontaneous pneumothorax, this is an unusual complication, according to Pablo Caro-Dominguez et al. The imaging study conducted by them, performed on 81 pediatric patients diagnosed with COVID-19, claims that in only 2% of patients the chest X-ray revealed spontaneous pneumothorax(14,15).
The literature describes a few pediatric cases of COVID-19 infection that associate spontaneous pneumothorax. From the information provided so far, this is the first pediatric case reported in a patient with chronic lung disease (asthma) who associated an infection with SARS-CoV-2 and developed spontaneous pneumothorax as a sequela of COVID-19 pneumonia.
The particularity of this case is the fact that the patient had a history (six months before developing pneumothorax) of COVID-19 mild lung infection on the background of an undiagnosed asthma at that time, with seemingly favorable immediate evolution, but with multiple severe respiratory complications that needed frequent presentation at the emergency room and hospitalization even in the conditions of initiating chronic antiasthmatic background therapy, but which the patient did not follow consistently. On the other hand, the development of pneumothorax was not related to mechanical ventilation in this patient, as reported in the current literature regarding most cases of pneumothorax in a pandemic context.
Conclusions
The COVID-19 pandemic continues to be a challenge for diagnosis and therapeutic management, especially in the new post-COVID-19 respiratory pathology, which is beginning to take shape. Although it is assumed that the pediatric population with asthma has a lower susceptibility and severity of symptoms in the SARS-CoV-2 infection compared to adults, there are also severe forms of the disease with a higher risk of complications on the long term, especially in those with partial or non-therapeutically controlled disease. Spontaneous pneumothorax could be one of the sequelae of COVID-19 pneumonia, but at the same time further studies are needed to understand whether in a pediatric patient with asthma, pneumothorax appears as a complication of the underlying disease in the context of a viral infection or as a manifestation of the SARS-CoV-2 infection.
Conflicts of interests: The authors declare no conflict of interests.
Bibliografie
-
Cucinotta D, Vanelli M. WHO Declares COVID-19 a Pandemic. Acta Biomed. 2020 Mar 19;91(1):157-160.
-
Hartmann-Boyce J, Gunnell J, Drake J, et al. Asthma and COVID-19: review of evidence on risks and management considerations. BMJ Evidence-Based Medicine. 2021;26:195.
-
Papadopoulos NG, Mathioudakis AG, Custovic A, et al. Childhood asthma outcomes during the COVID-19 pandemic: Findings from the PeARL multi-national cohort. Allergy. 2021;76:1765–1775.
-
Chatziparasidis G, Kantar A. COVID-19 in Children with Asthma. Lung. 2021 Feb;199(1):7-12.
-
Licari A, Marseglia GL. What are the considerations for treating pediatric asthma during the COVID-19 pandemic?. Expert Opinion on Pharmacotherapy. 2021;22(6):651-653.
-
Liuzzo Scorpo M, Ferrante G, La Grutta S. An Overview of Asthma and COVID-19: Protective Factors Against SARS-CoV-2 in Pediatric Patients. Front Pediatr. 2021;9:661206.
-
Castro-Rodriguez JA, Forno E. Asthma and COVID-19 in children: A systematic review and call for data. Pediatr Pulmonol. 2020 Sep;55(9):2412-2418.
-
CDC COVID-19 Response Team. Coronavirus Disease 2019 in Children - United States, February 12-April 2, 2020. MMWR Morb Mortal Wkly Rep. 2020 Apr 10;69(14):422-426.
-
Moeller A, Thanikkel L, Duijts L, et al. COVID-19 in children with underlying chronic respiratory diseases: survey results from 174 centres. ERJ Open Res. 2020;6:00409-2020.
-
Buonsenso D, Gatto A, Graglia B, Rivetti S, Ferretti S, Paradiso FV, Chiaretti A. Early spontaneous pneumothorax, pneumomediastinum and pneumorrhachis in an adolescent with SARS-CoV-2 infection. Eur Rev Med Pharmacol Sci. 2021;25(12):4413-4417.
-
Hollingshead C, Hanrahan J. Spontaneous pneumothorax following COVID-19 pneumonia. ID Cases. 2020;21:e00868.
-
12. López Vega JM, Parra Gordo ML, Diez Tascón A, Ossaba Vélez S. Pneumomediastinum and spontaneous pneumothorax as an extrapulmonary complication of COVID-19 disease. Emerg Radiol. 2020;27(6):727-730.
-
Sun R, Liu H, Wang X. Mediastinal emphysema, giant bulla, and pneumothorax developed during the course of COVID-19 pneumonia. Korean J Radiol. 2020;21:541-544.
-
Lin CH, Lin CL, Lin WC, Wei CC. Long-term risk of pneumothorax in asthmatic children: A 12-year population-based cohort study. Medicine. 2020;99:51(e23779).
-
Caro-Dominguez P, Shelmerdine SC, et al. Collaborators of the European Society of Paediatric Radiology Cardiothoracic Task Force. Thoracic imaging of coronavirus disease 2019 (COVID-19) in children: a series of 91 cases. Pediatr Radiol. 2020 Sep;50(10):1354-1368.

Hepatită cu virusul herpetic uman 6 la doi gemeni monozigoţi imunocompetenţi – prezentare de caz
Emilia Pop, Alina Grama, Beatrice Chirileasa, Alexandra Mititelu, Tudor Lucian Pop
Introducere. Virusul herpetic de tip 6 (HHV-6) cuprinde două subtipuri distincte, HHV-6 A şi HHV-6 B. Chiar dacă în majoritatea cazurilor HHV-6 determină o afectare uşoară la pacienţii imunocomp...
Etiologia insuficienţei hepatice acute la copii
Alina Grama, Tudor Lucian Pop
Insuficienţa hepatică acută (IHA) reprezintă o patologie cu o mortalitate foarte mare la nou-născuţi, sugari sau copii, în absenţa transplantului hepatic de urgenţă. ...
Tratamentul durerii acute la nou-născut – modalităţi terapeutice în unitatea de terapie intensivă neonatală
Valentin Munteanu, Ioana Alecsandra Munteanu, Iulia Ciongradi, Ioan Sârbu, Elena Hanganu, Elena Tarcă, Bogdan A. Stana, Maria Stamatin
Durerea la nou-născut este o realitate de care ne lovim zilnic în unitatea de terapie intensivă neonatală (NICU). Chiar dacă exist...
Hepatită cu virusul herpetic uman 6 la doi gemeni monozigoţi imunocompetenţi – prezentare de caz
Emilia Pop, Alina Grama, Beatrice Chirileasa, Alexandra Mititelu, Tudor Lucian Pop
Introducere. Virusul herpetic de tip 6 (HHV-6) cuprinde două subtipuri distincte, HHV-6 A şi HHV-6 B. Chiar dacă în majoritatea cazurilor HHV-6 determină o afectare uşoară la pacienţii imunocomp...
Utilizarea dispozitivelor electronice în prima copilărie (0-5 ani): beneficii educaționale, riscuri de neurodezvoltare și recomandări clinice bazate pe dovezi – o sinteză narativă
Adriana Mihai, Ileana-Katerina Ioniuc, Oana-Raluca Temneanu, Paula Popovici, Alice-Nicoleta Grudnicki, Alina Murgu
Copiii cu vârsta mai mică de 5 ani cresc imersați în medii digitale bazate pe ecrane într-o măsură fără precedent istoric....