Tusea cronică la copil – provocări
Chronic cough in children – challenges
Abstract
Introduction. Cough is the most common symptom for consultation with a family doctor in many European countries. Its persistence for a long time affects the patient’s quality of life. Case report. We present the case of a 13-year-old adolescent hospitalized for frequent, emitting, all day long, spastic cough started 7 months earlier and who did not recover from antibiotic and symptomatic treatment. The clinical examination of the respiratory tract was within normal limits. Asthma, the most common cause of chronic cough in adolescents, was ruled out by spirometry and evaluation of athopy. Posteronasal drops have been also ruled out by ENT examination, and bronchoscopy and the determination of Quantiferon TB allowed the refutation of a pulmonary tuberculosis, but also of foreign body aspiration. Upper digestive endoscopy confirmed the presence of minimal gastroesophageal reflux and identified a polypoid formation with a broad base of implantation in the cardia, later confirmed by thoracoabdominal CT and esogastric barium transit. Under treatment with a proton pump inhibitor, the evolution was favorable, with the remission of the polyp and of cough exacerbations. Conclusions. Chronic cough may be the single manifestation of gastroesophageal reflux potentiated by an inflammatory formation in the cardia.Keywords
spastic coughrefluxcardial polypRezumat
Introducere. Tusea reprezintă simptomul cel mai frecvent pentru consultaţia la medicul de familie în multe ţări din Europa. Persistenţa ei o perioadă îndelungată afectează calitatea vieţii pacientului. Prezentare de caz. Un adolescent de 13 ani este internat pentru tuse spastică frecventă, emetizantă, diurnă şi nocturnă, debutată cu şapte luni anterior şi care nu s-a remis sub tratament antibiotic şi simptomatic. Examenul clinic al aparatului respirator a fost în limite normale. Astmul, cea mai frecventă cauză de tuse cronică la adolescent, a fost exclus prin spirometrie şi evaluarea terenului atopic. Drenajul posteronazal a fost de asemenea exclus prin examen ORL, iar bronhoscopia şi determinarea Quantiferon TB au permis infirmarea unei tuberculoze pulmonare, dar şi a aspiraţiei de corp străin. Endoscopia digestivă superioară a confirmat prezenţa unui minim reflux gastroesofagian şi a identificat o formaţiune polipoidă cu bază largă de implantare la nivelul cardiei, confirmată ulterior prin CT toracoabdominal şi prin tranzit baritat esogastric. Sub tratament cu inhibitor de pompă de protoni, evoluţia a fost favorabilă, cu remisiunea formaţiunii şi a exacerbărilor de tuse. Concluzii. Tusea cronică poate reprezenta manifestarea unică a unui reflux gastroesofagian potenţat de o formaţiune cu caracter inflamator la nivelul cardiei.Cuvinte Cheie
tuse spasticărefluxpolipcardieIntroduction
Cough is the most common symptom for a general practitioner consultation in many European countries(1). Although it is well known that cough is a defense mechanism, its persistence for a long time affects the quality of life of the patient, especially when associated with comorbidities, such as urinary incontinence, dysphonia, syncope or vomiting(1,2). On average, 10-11 episodes of cough per day can be classified as normal, when the child does not show other associated symptoms(2). Between 35% and 40% of school-age children have a persistent cough for up to 10 days after the onset of an acute infectious episode, and preschool children may continue to cough for up to 25 days after an episode of upper respiratory tract infection(3).
There are no studies to rigorously define when cough can be labeled as chronic(1,3). According to the 2019 ERS Guide for chronic cough, it is defined as daily, diurnal and/or nocturnal cough, lasting more than 4 weeks after the end of the acute infectious episode or more than 8 weeks after its onset(1).
During childhood, the respiratory tract and the nervous system undergo a series of maturation processes that influence the cough reflex. Moreover, the immune response goes through developmental processes that make infections and birth defects important causes of cough(1,2,4).
Approximately 35% of preschool children had a prolonged cough at some point(1). Reports of the prevalence of chronic cough in the pediatric population vary, for example 1% of the pediatric population in India experience an episode of chronic cough, in China – 5-12%, and in Eastern Europe – 9%(1,3).
Some cases of chronic cough are a real challenge for the specialist, both in terms of diagnosis and therapeutic approach.
Case report
The authors present the case of a 13-year-old boy hospitalized in the pediatric clinic of “Grigore Alexandrescu” Emergency Clinical Hospital for Children in May 2019 for chronic, spastic, vomiting generating cough, worsened 24 hours before hospitalization.
Heredocollateral and personal physiological history did not provide significant information for the current condition. The personal pathological history includes: adenoidectomy in 2006, gastroesophageal reflux with esophagitis diagnosed in 2016, for which he received a complete treatment and it was endoscopically verified the favorable evolution. Exposure to noxious substances, dust or irritants has been ruled out.
The condition has been evolving for seven months, with the presence of four prolonged episodes of spastic cough with bloody sputum lasting 2-4 weeks. He was repeatedly evaluated and received antibiotics, bronchodilators and inhaled corticosteroids without the complete remission of cough. A new exacerbation suddenly installed raised the suspicion of foreign body aspiration and caused hospitalization.
The clinical examination revealed: elongated adolescent, T = 180 cm, G = 72 kg, BMI = 22.2 kg/m2, afebrile, frequent spastic cough, tiring, diurnal and occasionally nocturnal, without pulmonary auscultatory changes, normal cardiac examination, Sat O2 = 97-98%. Present, cooperative, without signs of meningeal irritation.
The investigations performed at hospitalization revealed: blood count with values within normal limits, without inflammatory syndrome, liver and kidney function within normal limits, nasal and pharyngeal cultures – negative. Clinical ENT evaluation: free nostrils, permeable sinus orifices, without obvious secretions.
The pulmonary X-ray exam (Figure 1) at admission showed a slightly accentuated bilateral infrahilar interstitial pattern, and the Quantiferon TB test was negative.

Pulmonary functional testing by spirometry was normal, without bronchial hyperreactivity syndrome. Also, the serum level of total IgE was normal and the panel of inhaled allergens was negative. Serologies for Mycoplasma pneumoniae and Chlamydia trachomatis were negative.
Bronchoscopy did not identify changes in the architecture of the tracheobronchial tree, secretions, bronchiectasis and invalidated the presence of foreign bodies in the airways. From the tracheobronchial aspirate, it did not develop BAAR or other pathogenic germs on specific culture media.
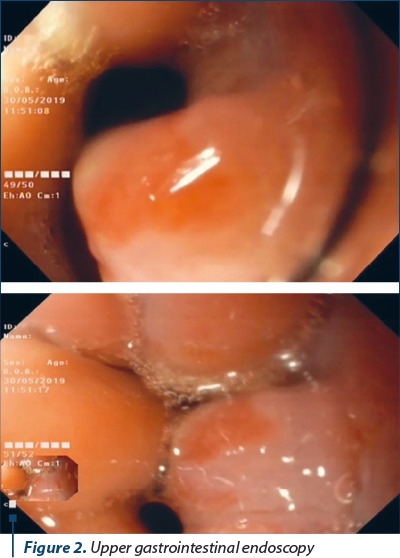
Upper digestive endoscopy (Figure 2) identified, at the level of the cardia sphincter, a nonbleeding polypoid formation with a diameter of 1 cm with a large base of implantation. Minimal gastroesophageal reflux. The test for Helicobacter pylori in the gastric mucosa fragment was negative.
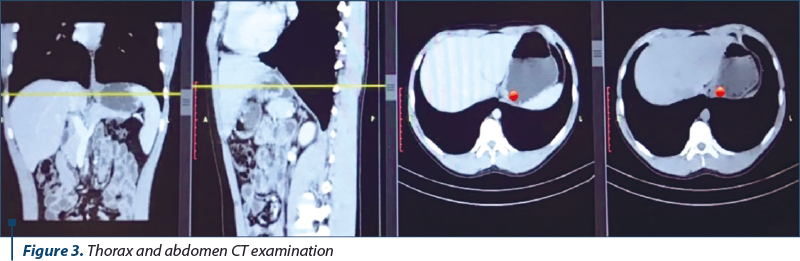
The thoracoabdominal CT examination (Figure 3) confirmed a polypoid formation located at the cardia sphincter, with homogeneous appearance (native and postcontrast) and discrete thickening of the gastric mucosa in the vicinity.
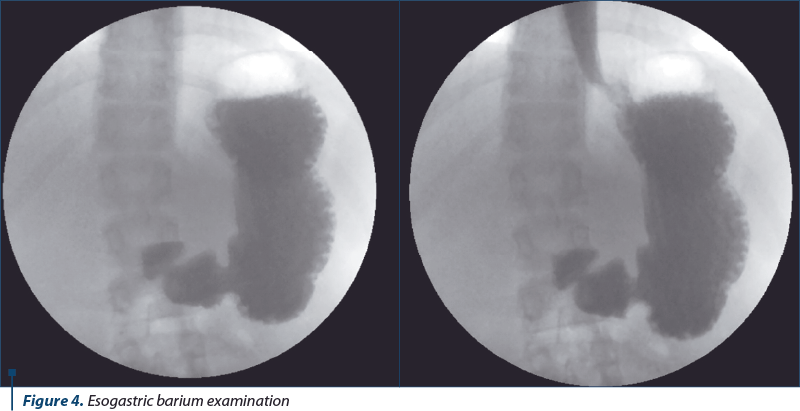
The esogastric barium transit (Figure 4) highlighted an esophagus with normal contour, caliber and motility, intermittent gastroesophageal reflux at the level of the cardial sphincter, normotonic, normokinetic stomach. The anatomopathological examination of the biopsy sample collected endoscopically from the formation identified a histological aspect that pleaded for the diagnosis of an inflammatory polyp (hyperplastic) of esogastric junction.
Discussion
The chronic cough of the child differs from that of the adult in terms of etiology and management. The initial assessment of cough requires a detailed history and a detailed clinical examination. Chest radiography and spirometry are essential elements in the diagnosis of chronic cough(1,4).
The most common causes of chronic cough are, according to the ERS, the triad allergic asthma, posteronasal drops and gastroesophageal reflux, but the morphological and functional peculiarities of the respiratory tract and the immunological dynamics specific to pediatric age should not be neglected(1,3,5).
There are at least nine systematic studies in adults regarding the etiology of chronic cough triad that covers the largest proportion of cases, which showed that posterior nasal drainage, asthma and GERD were responsible for 90-100% of cases of chronic cough in the immunocompetent adults. The same triad is relevant to children. Approximately 18-42% of patients have two causes of cough and up to 42% have three causes(1) (Table 1).

In front of an adolescent with chronic cough, with a prolonged, repetitive evolution, in our case over 7 months, with spastic, emitting, tiring character and with normal clinical examination of the respiratory system, there are multiple problems related to etiology and evaluation, on one hand, and therapy, on the other hand.
Normal ENT examination ruled out a possible posteronasal drainage. Day and night spastic cough with an evolution of more than three months may be suggestive of atypical pneumonia, a diagnosis ruled out by negative serologies for Chlamydia trachomatis and Mycoplasma pneumoniae.
An allergic asthma is excluded by the history of the condition, the normal serum level of total IgE and a panel of pneumoallergens were negative, with normal respiratory functional tests, both in rest and challenge. Moreover, the addition of beta-adrenergic bronchodilators and long-term inhaled corticosteroid therapy in exacerbations have not been shown to be effective in the short-term development and recurrence of episodes.
Foreign body aspiration, quite rare over the age of 6-7 years old, was ruled out by bronchoscopy, and the determination of Quantiferon TB and the absence of BAAR in the tracheobronchial aspirate allowed the exclusion of a pulmonary tuberculosis.
Upper digestive endoscopy for gastroesophageal reflux allowed its confirmation and the identification of a polypoid formation that accentuated it.
According to a study published in UpToDate in February 2021, gastric polyps are relatively common, found in about 6% of pediatric patients who undergo upper digestive endoscopy, and most are located in the fundic glands and antral mucosa and are associated with Helicobacter pylori infection, and only a very small part can be located in the cardia sphincter(6,7). At sizes up to 1.5 cm, they have no indication for endoscopic resection, but for conservative surgical treatment and drug treatment with proton pump inhibitor alone or in triple therapy, in case of Helicobacter pilory infestations(6,8).
The role of gastroesophageal reflux, esophageal dysmotility and aspiration in chronic cough is controversial. Its prevalence is estimated to be between 0 and almost 100%(1). On the other hand, frequent and persistent coughing fits may be responsible for increased intraabdominal pressure and exacerbation or even for the onset of gastroesophageal reflux. Many of the signs and symptoms associated with chronic cough can be explained by reflux and aspiration(1).
Hyperplastic polyps cover about 75% of gastric polyps, especially in areas where H. pylori infestation is common. Hyperplastic polyps are the result of epithelial hyperregeneration in response to preexisting chronic inflammatory stimulation(7). A polyp with a juxtacardial location impairs heart function and will accentuate or even cause recurrent episodes of persistent cough.
The patient received specific dietary recommendations and treatment with proton pump inhibitors and prokinetic medication for eight weeks. The short-term clinical evolution was favorable, with complete remission of cough episodes. In the long term, no other cough episodes were noticed in the patient’s dispensary at six months. Endoscopic reassessment at two months confirmed the remission of the cardiac formation.
The patient’s personal pathological history (gastroesophageal reflux one year before hospitalization) correlated with a favorable clinical evolution under treatment, confirmed by endoscopic control reassessment, supports the idea that chronic inflammatory stress of the gastric mucosa generated mucosal hyperplasia with gastroesophageal reflux and secondarily caused episodes of coughing.
Conclusions
In the case of a patient with recurrent, chronic or persistent cough and a history of gastroesophageal reflux with reflux esophagitis, it is necessary to repeat the upper digestive endoscopy. Of course, in a case of chronic cough, we will not consider the inflammatory polyp of the cardia as the first differential diagnosis, but an endoscopic evaluation of the upper digestive tract can be useful.
The presence of a juxtacardial localized polypoid formation raises the question of its etiology: it is a consequence of reflux that produces polypoid hyperplasia of the mucosa or is a polypoid formation independent of reflux, but which can aggravate its magnitude and clinical consequences, as well as chronic cough. Prolonged repetitive cough is the only manifestation of gastroesophageal reflux in an adolescent, which is not mentioned in any of the current pediatric guidelines.
Bibliografie
-
Morice A, Millqvist E, Bieksiene K, et al. ERS guidelines on the diagnosis and treatment of chronic cough in adults and children. European Respiratory Journal. 2020;55:1901136; DOI: 10.1183/13993003.01136-2019
-
Alsubaie H, Al-Shamrani A, Alharbi AS, et al. Clinical practice guidelines: Approach to cough in children: The official statement endorsed by the Saudi Pediatric Pulmonology Association (SPPA). International Journal of Pediatrics and Adolescent Medicine. 2015 March;2(1):38-43.
-
Hay AD, Wilson A, Fahey T, et al. The duration of acute cough in preschool children presenting to primary care: a prospective cohort study. Fam Pract. 2003 Dec;20(6):696-705.
-
de Jongste JC, Shields MD. Chronic cough in children. Thorax. 2003;58:998–1003.
-
Kasi A, Kamerman-Kretzmer RJ. Cough. Pediatrics in Review. 2019 Apr;40(4):157-167.
-
MacFarland SP, Zelley K, Katona BV, et al. Gastrointestinal Polyposis in Pediatric Patients. Journal of Pediatric Gastroenterology and Nutrition. 2019 Sep;69(3):273-280.
-
Mahachai V, Graham D, Odze R. FRCPC Gastric polyps, https://www.uptodate.com/contents/gastric-polyps/print. Feb 16, 2021.
-
Van Leerdam M, Roos V, van Hooft J, et al. Endoscopic management of polyposis syndromes: European Society of Gastrointestinal Endoscopy (ESGE) guideline. Endoscopy. 2019 Sep;51(9):877-895.

Prezentare de caz: sindrom VACTERL (malformaţii anorectale, cardiace şi renale)
Emilia Pop, Alina Grama, Alexandra Mititelu, Claudia Simu, Patricia Lorinţiu, Simona Căinap, Bogdan Bulata, Laura Bodea, Tudor Lucian Pop
Introducere. VACTERL este o patologie rară, a cărei denumire este compusă din acronimul malformaţiilor componente: anomalii...
Hepatită autoimună de tip 1 asimptomatică cu nivel normal al IgG şi deficit de IgA – prezentare de caz
Alexandra Mititelu, Alina Grama, Mihaela Spîrchez, Claudia Simu, Emilia Pop, Patricia Lorinţiu, Tudor Lucian Pop
Introducere. Hepatita autoimună (HAI) la copii este o boală hepatică cronică inflamatorie, cu un spectru clinic larg, de la o cre...
Spirometric assessment in asthma in children
Bogdan A. Stana, Awwab Shahid
Astmul este o boală importantă, atât la adulţi, cât şi la copii, care conduce frecvent la implicaţii financiare şi de sănătate semnificative la nivel global, afectând peste 300 de milioane de oameni din întreaga lume. Astmul este observat iniţial în copilărie şi se manifestă împreună cu afecţiuni precum f...
Spirometric assessment in asthma in children
Bogdan A. Stana, Awwab Shahid
Astmul este o boală importantă, atât la adulţi, cât şi la copii, care conduce frecvent la implicaţii financiare şi de sănătate semnificative la nivel global, afectând peste 300 de milioane de oameni din întreaga lume. Astmul este observat iniţial în copilărie şi se manifestă împreună cu afecţiuni precum f...
Suplimentele dietetice în practica pediatrică – prieteni sau duşmani pentru afecţiunile hepatice?
Iulia Ţincu, Ioana Maria Otilia Lică, Ana Maria Daviţoiu, Sorina Chindriş, Mirela Silvia Iancu, Ioana Adriana Ghiorghiu, Doina Anca Pleşca
Patologia hepatică cronică implică un management de caz extins, asociind frecvent un risc crescut de malnutriţie, ceea ce reprezin...