Tromboză spontană a arterelor femurale la un nou-născut – studiu de caz
Spontaneous femoral artery thrombosis in a newborn infant – case report
Abstract
Spontaneous femoral artery thrombosis in the neonate is rare. Often, the arterial thrombus in neonates is secondary to central line insertion or sepsis. Arterial thrombosis is associated with significant morbidity, unless promptly diagnosed and managed. In this case report, we highlight that a prompt recognition and management of arterial thrombosis in neonate led to a good outcome. In the treatment of this case, we have used milrinone, which is often used in the cardiac failure setting, as an agent to enhance peripheral circulation to help preserve tissue viability, because of its vasodilatory effect.Keywords
newbornarterial thrombosisRezumat
Tromboza arterială spontană la nou-născut este un eveniment rar întâlnit. De cele mai multe ori este secundară inserţiei de cateter vascular central sau infecţiei. Tromboza arterială asociază morbiditate semnificativă, în lipsa diagnosticului prompt şi a tratamentului de urgenţă. În acest raport de caz subliniem importanţa diagnosticului şi a intervenţiei rapide care au dus la un rezultat pozitiv. În tratamentul acestui caz am folosit milrinonă, un agent frecvent întâlnit în tratamentul insuficienţei cardiace, pentru a îmbunătăţi circulaţia periferică, cu scopul de a menţine viabilitatea ţesuturilor, datorită efectului său vasodilatator.Cuvinte Cheie
nou-născuttromboză arterialăBackground
Newborn infants are in a prothrombotic status because of immature coagulation system and exposure to prothrombotic factors(1,2). Spontaneous venous thrombosis is common and is often secondary to a central line placement.
Arterial thrombosis is usually a complication of umbilical arterial catheter placement and is often associated with sepsis. Spontaneous arterial thrombosis is very uncommon(3,4). Once diagnosed, arterial thrombosis of the extremity is a time critical lesion. The risk of limb loss is high, unless immediate measures are taken to prevent ischaemia and gangrene.
We report a case of spontaneous femoral artery thrombosis in a newborn infant who presented soon after birth, which threatened limb loss and was successfully managed.
Case presentation
A baby was born to a young primiparous mother at term, with a birth weight of 3.15 kg. Pregnancy was not complicated by any medical condition.
The mother was not on any medication during pregnancy, apart from vitamins. There was no significant family history.
Before delivery, the mother developed hypertension and a non-reassuring cardiotocography trace, therefore emergency caesarean section was performed. The baby was well at birth and did not need admission to the neonatal unit.
At four hours of age, it was noticed that the baby’s left leg was pale, mottled and cold, with reduced spontaneous movements. The left femoral pulse was feeble and pulses in the left foot were absent both clinically and by the Doppler. The rest of the systemic examination was unremarkable. The baby was admitted to the local neonatal unit.
Investigations
The baby had normal full blood count and coagulation tests. There was no polycythemia.
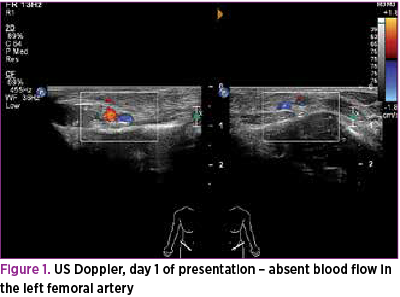
Renal function tests, liver function tests and bone profile were all normal. Doppler ultrasound scan of the left leg and groin confirmed the left common femoral artery thrombosis (Figure 1).
Cranial ultrasound scan was reported as normal and a detailed echocardiograph showed normal structure of the heart.
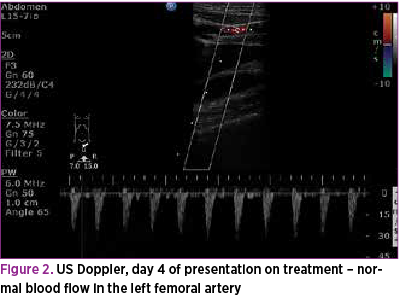
After four days of treatment, a repeated Doppler ultrasound scan revealed the complete resolution of the left common femoral artery thrombus (Figure 2). Protein S, protein C and anti-thrombin tests were not done as the presentation was not suggestive of these conditions and there was no family history. Blood gas showed no evidence of metabolic acidosis; hence, investigations for rare metabolic conditions were not performed. Blood culture and CRP were normal.
Differential diagnosis
The most common cause of an ischaemic limb in a neonate is the iatrogenic occlusion of an arterial blood supply. In this case, no central lines were in place prior to developing symptoms.
We considered a diagnosis of sepsis, and the baby was treated with antibiotics; however, the blood culture was negative and CRP was normal.
We considered deficiencies of protein C, protein S or anti-thrombin 3; however, this was not the usual presentation for these abnormalities, hence no further investigations were carried out. The potential in utero origin of the emboli was also discussed, however it could not be proven.
Treatment
The baby was started on nitro-glycerine cream topically to the left leg. Right leg was kept warm to stimulate sympathetic reflex.
The baby was started on antibiotics. The case was discussed with the vascular surgeons, and decision was made in favour of conservative management, in view of the technical challenges of embolectomy or thrombectomy which was deemed not necessary. After discussing with the haematologist, subcutaneous low molecular weight heparin was started at a dose of 1.5 mg/kg twice a day as anticoagulant. The baby was kept well hydrated with intravenous fluids and enteral feeding. The baby was also started on i.v. milrinone infusion at a dose of 0.2 micrograms/kg/minute as a systemic vasodilator to enhance the systemic perfusion. The baby did not receive a loading dose of milrinone to avoid unintentional fall in blood pressure.
There was a significant improvement in the clinical condition in the next few days with improved perfusion. Therefore, milrinone was stopped after 48 hours.
Antibiotics were also stopped after 48 hours as there was no evidence of sepsis. Low molecular weight heparin was stopped after seven days, as we noticed the full resolution of the thrombus on the repeated Doppler ultrasound scan.
Outcome and follow-up
By day 2, there was significant improvement of perfusion and circulation in the affected limb. By day 3, the left foot looked normal with good pulses.
On the fourth day of treatment, a repeated Doppler ultrasound scan of left common femoral artery revealed complete resolution of the clot with normal blood flow. When reviewed at nine months of age, the baby was doing very well.
Discussion
The spontaneous arterial occlusion is a rare event. Often, the cause for occlusion is unclear and it is difficult to differentiate whether it was due to a thrombus or emboli, and also whether the event was ante- or postnatal. There are few case reports and case series in literature focussing on etiology and management(5-9).
A Canadian registry reported 97 cases of neonatal thrombosis over a three-year period, from 29 centres. Out of these, 33 were neonates with arterial thrombosis. Among these 33 cases, most common reported sites were the femoral and iliac arteries in 16/33 (48%). The most common cause was sepsis, related to the line placement. The reported mortality was 21%; however, the mortality was not directly associated with the arterial thrombotic event.
In the rest of the cases, the cause of the arterial thrombosis was unclear(9). In a series of 32 neonates with thrombus from Netherland, there was no report of arterial thrombus(8). Both these studies suggest that the spontaneous arterial thrombus is an uncommon condition.
Known risk factors for vascular thrombosis are intravascular catheterisation, fetal thromboembolism (due to amniotic bands, death of one fetus in a twin pregnancy and maternal diabetes or sepsis), polycythemia, congenital heart disease and inherited deficiencies of antithrombin III and protein C.
The management includes anticoagulant treatment with heparin or low molecular weight heparin, thrombolytic treatment or surgery.
A recent systematic review provided no conclusions about the most appropriate treatment, as no eligible studies were found(10).
The treatment varies greatly among different centres due to the lack of evidence regarding the most appropriate management of the affected infants. In this case, combined treatment with topical nitroglycerine, milrinone infusion and enoxaparin helped to restore circulation in the affected limb. Milrinone is increasingly used in neonates for its vasodilator and inotropic effects. However, there are no reports of milrinone use in the management of arterial thrombosis in a neonate.
In conclusion, spontaneous femoral artery thrombosis is a rare condition. Early recognition and prompt initiation of treatment can lead to complete resolution of thrombus.
Learning points/take home messages
Spontaneous arterial thrombosis is rare in neonates. A high index of suspicion based on clinical signs and Doppler ultrasound aids early diagnosis.
Prompt treatment with anticoagulants and vasodilator therapy is life and limb saving.
Spontaneous arterial thrombosis in neonates is associated with significant morbidity and mortality.
Conflict of interests: The authors declare no conflict of interests.
Bibliografie
1. Armstrong AP, Page RE. Intrauterine vascular deficiency of the upper limb. J Hand Surg (Br).1997; 22: 607–611.
2. Beardsley DS. Venous thromboembolism in the neonatal period. Seminars in Perinatology. 2007; vol. 31, no. 4, pp. 250–53.
3. Letts M, Blastorah B, al-Azzam S. Neonatal gangrene of the extremities. J Paediatr Orthop. 1997; 17: 397–401.
4. Alpert J, O’Donnell JA, Parsonnet V et al. Clinically recognized limb ischemia in the neonate after umbilical artery catheterization. Am J Surg. 1980; 140(3):413e8.
5. Chalmers EA. Neonatal thrombosis. J Clin Pathol. 2000; 53:419–423.
6. Szvetko A, Hurrion E, Dunn A et al. Axillary Artery Thrombosis in a Neonate in Utero: A Case Report. Case Reports in Pediatrics. 2014; Article ID 417147.
7. Gürsu HA, Varan B, Oktay A et al. A case of neonatal arterial thrombosis mimicking interrupted aortic arch. Turk Pediatri Ars. 2015; 50: 118-22.
8. van Elteren HA, Veldt HS, te Pas AB et al. Management and Outcome in 32 Neonates with Thrombotic Events. International Journal of Pediatrics. 2011; Article ID 217564.
9. Schmidt B, Andrew M. Neonatal Thrombosis: Report of a Prospective Canadian and International Registry. Pediatrics. 1995; 96, 939.
10. John CM, Harkensee C. Thrombolytic agents for arterial and venous thromboses in neonates. Cochrane Database Syst Rev. 2005.

Prognosticul materno-fetal şi managementul bolilor inflamatorii intestinale în sarcină
Andreea Boiangiu, Cristian Tiereanu, George Alexandru Filipescu, Cristina Maria Miron, Simona Vlădăreanu
Bolile inflamatorii intestinale (rectocolita ulcerohemoragică, boala Chron, colite neprecizate) afectează femeile tinere de vârstă fertilă, ducând la o provocare a obţinerii unei sarcini sănătoase. El...
Sindrom de colestază neonatală la un prematur cu greutate foarte mică la naştere (VLBW) – prezentare de caz
Elena Andreea Ştioiu, Iustina Beşleagă, Diana Costache, Simona Popescu, Iulia Petrescu, Simona Vlădăreanu
Sindromul de colestază neonatală reprezintă o patologie importantă (cu o incidenţă de 1/2500 de nou-născuţi vii), care ridică mult...
Prognosticul materno-fetal al sarcinii complicate cu ciroză biliară secundară – review al literaturii de specialitate şi prezentare de caz
Andreea Boiangiu, George Alexandru Filipescu, Georgiana Dinu, Radu Vlădăreanu, Simona Vlădăreanu
Managementul gravidei cu afectare hepatică reprezintă o adevărată provocare pentru echipa complexă formată din obstetrician, gastr...
Artrogripoza la un nou-născut prematur provenit din sarcină gemelară. Prezentare de caz
Ana Maria Măreşescu, Simona Vlădăreanu, Ana Maria Brădeanu, Adriana Tecuci, Simona Popescu
Artrogripoza congenitală multiplă (AMC) este caracterizată în literatura de specialitate de multiple contracturi articulare congenitale la nou-născut. Amioplazia este cea mai frecventă formă de AMC şi...
Malformaţiile congenitale de tub digestiv: duplicaţie intestinală toraco-abdominală – prezentare de caz
Claudia Kosztelnik, Aurelia Tanca, Irina Bachis, Mihaela STAICU, Dorina Tudor
Malformațiile congenitale ale tubului digestiv, precum duplicațiile intestinale, sunt entități rare, cu o variabilitate morfologică și topografică semnificativă. ...