Postpartum hemorrhage – a major obstetrical emergency. Causes and treatment
Hemoragia în post-partum – o urgenţă obstetricală majoră. Cauze şi tratament
Abstract
Introduction. Postpartum hemorrhage (PPH) is a significant maternal health concern, representing a major cause of obstetric mortality globally. Materials and method. In this retrospective study, we analyzed cases of postpartum hemorrhage, from April 2019 to April 2021, from the “Bucur” Maternity, Bucharest. Results. This study included 100 cases of postpartum hemorrhage. Among them, 30 occurred after caesarean sections and 70 occurred following vaginal deliveries. The identified causes of PPH after caesarean section were uterine atony (90%), placental retention (6.66%) and uterine rupture (3.33%). For PPH after vaginal delivery, uterine atony was identified as the most common cause in 38 patients. Multiparity was the most frequent cause of uterine atony. Conclusions. The most common cause of postpartum hemorrhage was uterine atony, being more frequent after caesarean section. SARS-CoV-2 infection correlated with an increased frequency of uterine atony and postpartum hemorrhage.Keywords
postpartum hemorrhageuterine atonycaesarean sectionRezumat
Introducere. Hemoragia post-partum (HPP) este o problemă semnificativă de sănătate maternă, reprezentând o cauză majoră de mortalitate obstetricală la nivel global. Materiale şi metodă. În acest studiu retrospectiv, am analizat cazuri de hemoragie post-partum, din aprilie 2019 până în aprilie 2021, de la Maternitatea „Bucur”, Bucureşti. Rezultate. Studiul de faţă a inclus 100 de cazuri de hemoragie post-partum, dintre care 30 au apărut după cezariană şi 70 după naşteri vaginale. Cauzele identificate ale HPP după cezariană au fost atonia uterină (90%), retenţia placentară (6,66%) şi ruptura uterină (3,33%). În cazul HPP după naşterea vaginală, atonia uterină a fost identificată ca fiind cea mai frecventă cauză, la 38 de paciente. Multiparitatea a fost cea mai comună cauză a atoniei uterine. Concluzii. Cea mai frecventă cauză a hemoragiei post-partum a fost atonia uterină, fiind mai frecventă după operaţia cezariană. Infecţia cu SARS-CoV-2 s-a corelat cu o frecvenţă crescută a atoniei uterine şi a hemoragiei post-partum.Cuvinte Cheie
hemoragie post-partumatonie uterinăoperaţie cezarianăIntroduction
Postpartum hemorrhage (PPH) represents a major maternal health issue, being one of the leading causes of maternal mortality globally, accounting for over half of maternal deaths occurring within the first 24 hours after childbirth(1). The incidence of postpartum hemorrhage varies between 5% and 15% of parturients, being defined as the bleeding occurring in the third and fourth stages of labor that exceeds 500 ml for vaginal birth and 1000 ml for caesarean section(2). Due to the often imprecise assessment of bleeding, PPH can also be defined as bleeding leading to a decrease in hematocrit by more than 10% or as bleeding requiring correction through transfusion(3).
The causes of PPH are divided based on the stage of childbirth when it occurs. In the third stage, the cause may be retained placenta, while in the fourth stage, the causes of PPH can include retained placental fragments or uterine atony. Additionally, pelvic-genital traumatic injuries or coagulopathies can be causes of PPH in both stages(4).
There are numerous risk factors for PPH, including polyhydramnios, multiple pregnancies, precipitous or prolonged labor, chorioamnionitis, uterine malformations, multiparity, placenta praevia, abnormal placental adherence, cervical, vaginal or perineal injuries, uterine rupture or inversion, and coagulation disorders(5). However, there are multiple cases where PPH occurs in the absence of any risk factors, with the control of postpartum hemorrhage primarily depending on uterine contractions, and to a lesser extent on the activation of the coagulation cascade or other factors.
This study aims to highlight the experience of our clinic regarding PPH, based on patients’ characteristics, causes of PPH, treatment and outcome.
Materials and method
This is a retrospective, observational and analytical study realized in the “Bucur” Maternity which is the Obstetrics-Gynecology Department of the “Sf. Ioan” Emergency Clinical Hospital, Bucharest, from April 2019 to April 2021. It included a randomized analysis of postpartum hemorrhage cases. The study population consisted of 100 patients whose medical records, laboratory results and operative protocols were analyzed.
The following parameters were evaluated: patients’ age, admission symptoms, obstetrical history, mode of delivery, gestational age, fetal presentation, fetal birth weight, Apgar score, preexisting maternal conditions, SARS-CoV-2 infection, tobacco use during pregnancy, length of postpartum hospitalization, Rh incompatibility, complications during pregnancy, complications during childbirth, postpartum complications, episiotomy, causes of postpartum hemorrhage, presence of uterine scar, management of postpartum hemorrhage – pharmacological treatment (uterotonics administered, fluid therapy, blood transfusion), non-surgical treatment (uterine tamponade, manual or instrumental control of uterine cavity), surgical treatment (suturing lacerations, compressive sutures, vascular ligatures, hysterectomy) and, also, laboratory tests.
The collected data were centralized and analyzed using the IBM SPSS Statistics software version 28.
Results
The present study included 100 cases of postpartum hemorrhage. Among them, 30 occurred after caesarean sections and 70 occurred following vaginal deliveries. Among the vaginal deliveries, 63 were spontaneous cranial presentation births, two were breech presentations assisted with Bracht maneuver, and five were spontaneous home births that resulted in hospitalization due to massive hemorrhage during the fourth stage of labor.
The patients included in the study were between 17 and 44 years old, with an average age of 31 years old. Of these, 20% were primiparous and 80% were multiparous, with an average parity of five pregnancies. The mean gestational age was 37.5 weeks, with the lowest being 26 weeks, in two patients. In one of these two cases, there was placenta accreta leading to postpartum tissue retention and massive bleeding.
During the study period, there were 70 cases with PPH after vaginal delivery, with uterine atony identified as the most common cause, in 38 patients. In the study, multiparity was identified as the most frequent cause of uterine atony, while in six cases, uterine atony occurred without an identified cause.
The second most common cause were lesions, which occurred in 22 cases. Obstetrical lesions included perineal lacerations (12 cases), cervical ruptures (seven cases), and vaginal lacerations (three cases). Surgical treatment with suturing of the lacerations was performed in all cases, with favorable outcomes.
Placental retention was identified in seven patients which required instrumental uterine cavity control in five of them and hematological abnormalities correction in two cases.
For patients with uterine atony after vaginal delivery, the conservative management involved additional uterotonics and uterine massage. Bimanual uterine massage was performed in 10 patients, Bakri balloon and Foley catheter were used in two cases each, and hysterectomy for hemostasis was performed in two patients. Blood transfusions were administered in four cases, while fresh frozen plasma and platelet transfusion were used in two cases.
In this study, 30 cases of PPH were identified following caesarean section. The identified causes of PPH were uterine atony (90%), placental retention (6.66%) and uterine rupture (3.33%).
Among the factors for uterine atony in caesarean sections, there were identified 15 cases of placenta praevia, six cases of abruptio placentae, one case of uterine rupture, and two cases with placenta accreta. The conservative management was efficient in 20 cases of 27 patients with hemorrhage following caesarean section due to uterine atony. B-Lynch sutures were used in one case, Foley catheter was used in two cases, and O’Leary ligature in one case. Hysterectomy for hemostasis was performed in two patients: in the first case, uterine atony was caused by lateral placenta praevia in a primigravida patient with no other identifiable risk factors, and the second hysterectomy for hemostasis was performed in a 30-year-old patient at 30 weeks of pregnancy with abruptio placentae.
Placental retention was identified as the cause of PPH in two cases, both involving placenta accreta. It was identified a uterine rupture in a 29-year-old patient at 38 weeks of pregnancy with previous caesarean scar. The treatment was represented by hysterorrhaphy.
Using the classification developed by the California Maternal Quality Care Collaborative, the patients included in the study were categorized into three groups, based on various factors, for the estimation of the risk of developing postpartum hemorrhage (low, medium, or high risk).
Out of the 100 patients who experienced PPH, 66% of them were identified as being in a risk group, with 33% in the high-risk group. The remaining 34 patients had no identifiable pre-PPH risk factors.
Patients who experienced PPH after vaginal delivery were predominantly identified in the medium-risk group (29 out of 70 patients), with the most common factor being multiparity (having more than four previous vaginal deliveries). This correlates with the fact that the overall study group had an average of five pregnancies, and multiparity is a well-known risk factor for uterine atony and PPH.
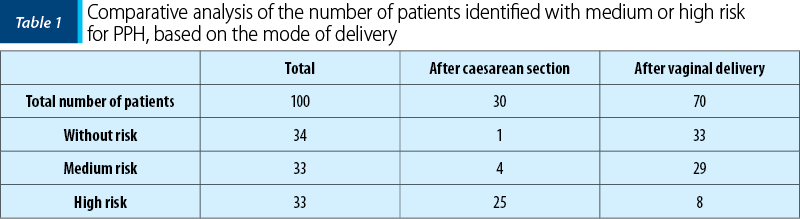
On the other hand, patients who gave birth by caesarean section had a predominantly high risk (25 out of 30 patients). This result was predictable because the risk factors (placenta praevia, placenta accreta) were the indications for caesarean section.
Table 2 presents the correlations between patients’ risk of developing PPH (risk calculated using the CMQCC classification) and various variables. It reveals a positive correlation with the mode of delivery, meaning that patients with a high risk mostly gave birth by caesarean section. We highlight the positive correlation between SARS-CoV-2 infection and the risk, indicating that the majority of patients infected with SARS-CoV-2 were categorized into the high-risk group for PPH.

SARS-CoV-2 infection was identified in 13 patients in the entire cohort (13%).
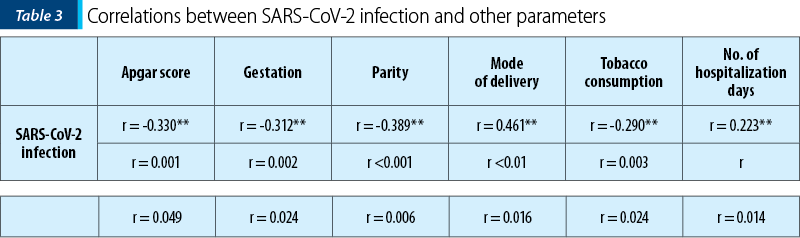
Regarding SARS-CoV-2 infection in patients with PPH, we identified the following relevant correlations: there was a negative relationship between the Apgar score and SARS-CoV-2 infection, meaning that in COVID-19 the Apgar score of the newborns was lower. Additionally, it appears that there is a negative relationship between gestation, parity and SARS-CoV-2 infection, specifically that infection was predominantly present in individuals with lower gestation and parity. On the other hand, the relationships between the mode of delivery, the number of days of hospitalization and SARS-CoV-2 infection were positive, meaning that the infection was predominantly present in PPH patients who gave birth by caesarean section and had a longer hospital stay. The relationship between tobacco use and SARS-CoV-2 infection was negative, indicating that nonsmokers were predominantly infected.
Discussion
Postpartum hemorrhage remains the primary cause of maternal morbidity and mortality in Romania. Globally, it represents the leading preventable cause of maternal morbidity and mortality(2). The new management protocols, medications and treatment modalities have improved the patients outcomes and reduced the number of complications in postpartum hemorrhage.
In this study, we analyzed the maternal outcomes of 100 patients discharged with a primary diagnosis of postpartum hemorrhage (period III or IV). These 100 cases represent approximately 2.5% of all births that occurred during the analyzed period in the “Bucur” Maternity (in the literature, the percentage varies from 2% to 10%)(3).
In the entire study cohort, there were no maternal deaths or reinterventions after discharge. Hysterectomy for hemostasis was performed in four patients (4% of cases) of PPH for uterine atony. These results are consistent with those from the specialized literature, which recognizes atony and uterine rupture as the most common causes for emergency hysterectomy. More recent reports also include placenta accreta as a frequent factor(6).
The most frequent cause of postpartum hemorrhage in our study was uterine atony, being present in 65% of cases. This percentage varied depending on the type of delivery – after vaginal delivery, 53.2% of cases were attributed to uterine atony, while after caesarean section, 90% of cases were due to uterine atony. This percentage is lower than the one found in literature, as atony is described as responsible for at least 75% of cases of postpartum hemorrhage cases(7).
The causes of uterine atony were various, multiparity being the most common cause in the group of patients who gave birth vaginally (in nine cases), while in the group of patients who gave birth by caesarean section, placenta praevia was the predominant cause of PPH (in 15 cases). These are well-established risk factors for uterine atony. However, a substantial proportion of postpartum atony occurs without any identified risk factors or causes(8).
Reducing morbidity among women with severe postpartum hemorrhage could be achieved when quantitative estimations of blood loss are used as a component of maternal safety protocols. However, a recent Cochrane review and meta-analysis did not show evidence that quantitative blood loss estimation reduces the need for uterotonics, blood transfusions, or the use of volume expanders during postpartum hemorrhage(9).
In cases of postpartum hemorrhage caused by uterine atony, the first step in the management is bimanual uterine massage, which is used to stimulate endogenous prostaglandins(10).
Pharmacological treatment was used postpartum in all patients diagnosed with postpartum hemorrhage. This consisted in prophylactic or simultaneous administration of uterotonics with uterine massage. This conservative management of postpartum atony was overall effective in treating 80% of cases, with a higher success rate in patients who gave birth vaginally (84.21%) compared to those who gave birth by caesarean section (74.07%). The primary uterotonics used were oxytocin (administered intravenously or intramuscularly) and ergometrine in most situations, except for cases with contraindications for ergometrine (hypertension), where oxytocin was used. This prioritized use aligns with the international studies. In a meta-analysis conducted in 2018, the best results in treating postpartum hemorrhage were seen with the combination of ergometrine + oxytocin, carbetocin, or misoprostol(10,11).
In our study cohort, the Bakri balloon was used in a case of post-vaginal delivery uterine atony. On the other hand, Foley catheters were used in three cases, one case after vaginal delivery atony and two cases after caesarean section atony. In all identified cases, these methods were sufficient to stop postpartum hemorrhage. In a meta-analysis that included over 4700 patients with postpartum hemorrhage, the success rate of uterine tamponade with the Bakri balloon was 85.9% overall. The response was more effective when the balloon was used after vaginal delivery (87%) compared to its use after caesarean section (81.7%)(12). In our study, these treatment methods (Bakri balloon or Foley catheter) were used in a very small percentage of cases, but they had a 100% effectiveness in the cases where they were applied. This difference in results from the study’s patient cohort is much smaller compared to the number of patients in the meta-analysis conducted by Suarez et al.(11)
Interesting results emerged from correlations regarding SARS-CoV-2 infection since the “Bucur” Maternity became a hospital dedicated to pregnant patients infected with SARS-CoV-2. Positive patients with this virus were admitted from March 2021. In the patient group analyzed, SARS-CoV-2 infection was present in 13% of cases. In these patients, the cause of postpartum hemorrhage was predominantly uterine atony, with only one case related to placental retention. Furthermore, SARS-CoV-2 infection during pregnancy was more frequent in patients identified in the high-risk group for postpartum hemorrhage and in patients who gave birth by caesarean section. This correlates with the amount of saline solution administered to SARS-CoV-2 positive patients which was higher compared to SARS-CoV-2 negative patients.
Moreover, our study shows that SARS-CoV-2 infection correlated negatively with the Apgar score, meaning that the infection was present in mothers who gave birth to infants with lower Apgar scores. Additionally, the infected patients required a longer hospital stay. The infection was more frequent in nonsmokers. Studies have demonstrated a direct relationship between coronaviruses and spontaneous abortion, preterm birth, intrauterine growth restriction and disseminated intravascular coagulation(13). Some studies suggest that COVID-19 is associated with increased rates of preterm birth, the need for caesarean section and with lower Apgar scores(13-15). Another retrospective study proved that SARS-CoV-2 infection does not correlate with an increased risk of postpartum hemorrhage or with higher morbidity. The same study identified that pregnancies with SARS-CoV-2 had a higher incidence of premature birth and severe preeclampsia(16).
Conclusions
The most common cause of postpartum hemorrhage identified in our study was uterine atony. Uterine atony was more frequent after caesarean section. Postpartum hemorrhage can occur in patients without identified risk factors. SARS-CoV-2 infection correlated with an increased frequency of uterine atony and postpartum hemorrhage. The conservative management in the treatment of postpartum atony was more effective in patients who gave birth vaginally, compared to those who gave birth by caesarean section.
Conflict of interest: none declared.
financial support: none declared.
This work is permanently accessible online free of charge and published under the CC-BY licence.

Bibliografie
-
Christopher L. A textbook of postpartum hemorrhage, Vital statistics – an overview. Dapiens Publishing, 2006;11-35, 55-8.
-
SOGC. Management of the third stage of labour to prevent postpartum hemorrhage. 2003;136:1-3.
-
Sentilhes L, Vayssière C, Deneux-Tharaux C, et al. Postpartum hemorrhage: guidelines for clinical practice from the French College of Gynaecologists and Obstetricians (CNGOF). Eur J Obstet Gynecol Reprod Biol. 2016;198:12-21.
-
Cunningham FG. Obstetrical Hemorrhage, Chapter 35. Williams Obstetrics, 24th Ed., 2014;780-828.
-
Jacobs AJ. Causes and treatment of postpartum hemorrhage. UpToDate. 2006;1-13.
-
Ende HB, Lozada MJ, Chestnut DH, et al. Risk factors for atonic postpartum hemorrhage: a systematic review and meta-analysis. Obstet Gynecol. 2021;137(2):305–23.
-
Diaz V, Abalos E, Carroli G. Methods for blood loss estimation after vaginal birth. Cochrane Database Syst Rev. 2018;9((9):CD010980.
-
Hofmeyr GJ, Abdel-Aleem H, Abdel-Aleem MA. Uterine massage for preventing postpartum haemorrhage. Cochrane Database Syst Rev. 2013;7:CD006431.
-
Mousa HA, Cording V, Alfirevic Z. Risk factors and interventions associated with major primary postpartum hemorrhage unresponsive to first-line conventional therapy. Acta Obstet Gynecol Scand. 2008;87(6):652–61.
-
Gallos ID, Papadopoulou A, Man R, et al. Uterotonic agents for preventing postpartum haemorrhage: a network meta‐analysis. Cochrane Database Syst Rev. 2018;4(4):CD011689.
-
Suarez S, Conde-Agudelo A, Borovac-Pinheiro A, et al. Uterine balloon tamponade for the treatment of postpartum hemorrhage: a systematic review and meta-analysis. Am J Obstet Gynecol. 2020;222(4):293.e1-293.e52.
-
Schwartz DA, Graham AL. Potential maternal and infant outcomes from coronavirus 2019-nCoV (SARS-CoV-2) Infecting pregnant women: lessons from SARS, MERS, and other human coronavirus infections. Viruses. 2020;12(2):194.
-
Qiao J. What are the risks of COVID-19 infection in pregnant women? Lancet Lond Engl. 2020;395(10226):760–2.
-
Liu C, Andrusier M, Silver M, Applewhite L, Clare CA. Effect of SARS-CoV-2 Infection on pregnancy outcomes in an inner-city black patient population. J Community Health. 2021;46(5):1029–35.
-
Wang MJ, Schapero M, Iverson R, Yarrington CD. Obstetric hemorrhage risk associated with novel COVID-19 diagnosis from a single-institution cohort in the United States. Am J Perinatol. 2020;37(14):1411–6.
-
Wang Y, Wang Y, Han X, Ye J, Li R. Potential effect of COVID-19 on maternal and infant outcome: lesson from SARS. Front Pediatr. 2020;8:511.

Clear cell carcinoma arising from endometriotic ovarian cyst
Maria Olinca, Anca Potecă, Elvira Brătilă, Mihai Mitran
Carcinomul cu celule clare este un subtip rar şi agresiv de cancer ovarian. Este adesea asociat cu endometrioza, o afecţiune cronică ce este caracterizată prin prezenţa de ţesut asemănător endometrului în afara uterului....
Fetal and neonatal diagnosis and management in a case of a neonate with congenital heart disease – case report
Maria-Andreea Răcean, Manuela Cucerea, Claudiu Mărginean, Liliana Gozar
Boala cardiacă congenitală (BCC) este cea mai frecventă formă de anomalie congenitală. La făt, canalul arterial (CA) deviază sângele neoxigenat din artera pulmonară în aorta descendentă. Majoritatea f...
Endometrial cancer and Lynch syndrome: similarities and genetic determinism
Robert Botea, Nicolae Suciu, Mădălina Piron-Dumitraşcu, Simona-Raluca Iacoban, Dragoş Creţoiu, Ioan Dumitru Suciu
Sindromul Lynch (SL), denumit anterior cancer colorectal ereditar nonpolipozic (HNPCC), este un tip de boală ereditară care este de natură autozomal dominantă. Această afecţiune este cauzată de pre...
A rare case of complete hydatidiform mole with prolonged evolution – clinical case
Mona Akad, Răzvan Socolov, Raluca Bălan, Diana Popovici, Eduard Crauciuc, Roxana Covali, Fawzy Akad, Tudor Buţureanu, Ana-Maria Apetrei, Alina Andriucă, Demetra Socolov
Mola hidatiformă, cunoscută drept sarcină molară, reprezintă o boală gestaţională trofoblastică cu punct de plecare placentar şi c...
Screening for cardiac anomalies in the first and second trimesters – diagnosing challenging cases
Alexandru Cristian Comănescu, Maria Cristina Comănescu, Nicolae Cernea, Agnesa Preda, Aura-Iuliana Popa
Screeningul pentru anomalii cardiace reprezintă o componentă critică a îngrijirii prenatale contemporane, necesitând o abordare proactivă pentru identificarea defectelor cardiace congenitale la f...