Conduita terapeutică a bolii tromboembolice în sarcină şi lăuzie
The management of thromboembolic disease in pregnancy and puerperium
Abstract
Pregnancy and particularly postpartum period associate a high risk of thromboembolic disease, especially when another procoagulant condition is present. Besides the hypercoagulable state characteristic to pregnancy, the factors that increase this risk are venous stasis of the lower extremities, endothelial injury, and the presence of an inherited thrombophilia. The thromboembolic risk grows exponentially during pregnancy and persists 12 weeks postpartum. Regarding the localization, there is a predisposition for developing deep vein thrombosis in left inferior limb, characteristic for 70% to 90% of cases, this predisposition being augmented by the hospitalization status. A history of venous thromboembolism associates a recurrence risk in pregnancy 20-30 times higher than the incidence of this pathology in pregnant and postpartum population. About 50% of venous thromboembolism in pregnancy associates hereditary or acquired thrombophilias; in this context, the screening for thrombophilic disorders should be recommended to all pregnant women who associate a history of venous thromboembolism or manifested venous thrombosis during the current pregnancy. For all cases of pregnancies and postpartum women, avoidance of dehydration, active live and, respectively, early mobilization are recommended. For the cases of pregnancies with confirmed antiphospholipid syndrome (APS), low doses of aspirin are recommended to be added to the prophylactic therapy with LMWH/UFH, as early as possible in pregnancy, up to 36 weeks of gestation, this treatment schedule having the highest efficiency in early pregnancy loss prevention and favorable pregnancy outcome. The cases of thromboembolism during pregnancy and puerperium are complex, with high mortality and morbidity risk, and require team collaboration between cardiologist, gynecologist, hematologist and intensive care specialists. The key to success for a good prognosis is the compliance with a clear, standardized, adapted protocol.Keywords
pregnancythromboembolismprophylaxisRezumat
Sarcina şi în special perioada post-partum asociază un risc crescut de boală tromboembolică, mai ales dacă este prezentă o altă condiţie procoagulantă. În afară de starea hipercoagulabilă caracteristică sarcinii, factorii care cresc acest risc sunt staza venoasă a extremităţilor inferioare, leziunile endoteliale şi prezenţa unei trombofilii moştenite. Riscul tromboembolic creşte exponenţial în timpul sarcinii şi persistă 12 săptămâni post-partum. În ceea ce priveşte localizarea, există o predispoziţie pentru dezvoltarea trombozei venoase profunde la nivelul membrului inferior stâng, caracteristică pentru 70% până la 90% din cazuri. Antecedentele de tromboembolism venos asociază un risc de recurenţă în timpul sarcinii de 20-30 de ori mai mare decât incidenţa acestei patologii la gravide şi în post-partum. Aproximativ 50% din tromboembolismul venos din timpul sarcinii se asociază unei trombofilii ereditare sau dobândite; în acest context, screeningul pentru tulburări trombofilice ar trebui recomandat tuturor femeilor gravide care asociază un istoric de tromboembolism venos sau tromboză venoasă manifestă în timpul sarcinii actuale. Pentru toate cazurile de sarcină şi lăuzie, se recomandă evitarea deshidratării şi mobilizarea activă şi precoce. Pentru cazurile de sarcină cu sindrom antifosfolipidic confirmat, la tratamentul profilactic cu LMWH/UFH se recomandă a fi adăugată aspirină în doză mică încă de la începutul sarcinii, până la 36 de săptămâni de gestaţie. Această schemă de tratament are cea mai mare eficacitate în prevenirea avorturilor spontane şi pentru rezultatul favorabil al sarcinii. Cazurile de tromboembolism în timpul sarcinii şi lăuziei sunt complexe, cu un risc crescut de mortalitate şi morbiditate, şi necesită colaborare interdisciplinară între cardiolog, ginecolog, hematolog şi specialişti în terapie intensivă. Cheia succesului pentru un bun prognostic este respectarea unui protocol clar, standardizat şi adaptat.Cuvinte Cheie
trombembolismsarcinăprofilaxieIntroduction
Pregnancy and particularly postpartum period associate a high risk of thromboembolic disease, especially when another procoagulant condition is present. Besides the hypercoagulable state characteristic to pregnancy, factors that increase this risk are venous stasis of the lower extremities, endothelial injury, and the presence of an inherited thrombophilia(1). Vascular trauma occurs mainly in labor, especially after instrumental vaginal delivery or after caesarean section, therefore during the first three months after birth the risk of venous thromboembolism is 60 times higher compared to the general population(1). Venous thromboembolic disease refers to deep vein thrombosis, pulmonary embolism and stroke; all of these pathologies have severe repercussions and are life-threatening(2). In the 21st century, pulmonary thromboembolism is one of the main causes of maternal death alongside with preeclampsia, obstetric hemorrhage, amniotic fluid embolism and cardiac disease(1), being responsible for about 9% of maternal deaths(2). The incidence of venous thromboembolism in pregnancy is 1/1600(3) and it can manifest as a deep vein thrombosis of a lower extremity, isolated, or as a pulmonary embolism(4). In the last decades, an important decrease in the incidence of venous thromboembolism in the postpartum period was observed(5), which is mainly attributed to the use of thromboprophylaxis. Further, we will describe the principle of thromboprophylaxis in pregnancy and postpartum period, the treatment of thromboembolic disease in pregnancy and postpartum period, anticoagulation during labor, and aspects of the anesthesia for anticoagulated pregnant women.
1. Fitting the pregnant woman into the high-risk group for thromboembolic disease
The thromboembolic risk grows exponentially during pregnancy and persists 12 weeks postpartum. Regarding the localization, there is a predisposition for developing deep vein thrombosis in left inferior limb characteristic for 70% to 90% of cases, this predisposition being augmented by the hospitalization status(6). All hospitalized pregnant women and women in puerperium must be clinically investigated for the associated risk of thrombotic disease. Arterial thrombosis occur exceptionally, and most frequently implicated sites are retina, subclavian artery or middle cerebral artery. The risk factors for thromboembolic disease in pregnancy and postpartum are divided in three categories, respectively(7):
-
Antepartum risk factors
1. personal history of thromboembolic disease
2.major hereditary thrombophilias (factor V Leiden, G20210A prothrombin gene mutation, antithrombin III deficiency, protein C and protein S)
3.antiphospholipid syndrome (APS)
4.medical comorbidities (e.g., oncological/haematological pathology with hyperviscosity, heart failure, valvular prosthesis, type 1 diabetes with nephropathy, nephrotic syndrome, systemically active lupus erythematosus, inflammatory bowel disease, rheumatoid arthritis, current intravenous medication, myeloproliferative diseases)
5.obesity (BMI≥30 kg/m2) before or at the onset of pregnancy
6. age ≥35 years old
7. parity ≥3
8. smoking
9.voluminous venous varicose veins (symptomatic/extended above the knee/associated with phlebitis, edema or skin changes)
10. paraplegia.
-
Obstetrical risk factors
1. multiple pregnancy
2. preeclampsia/eclampsia
3.emergency/elective caesarean section
4.instrumental delivery/ obstetrical maneuvers/ prolonged labor (>24 hours)
5. intrauterine fetal death
6. premature birth
7.postpartum hemorrhage (>1l/transfusion requiring).
- Transient/additional risk factors
1. surgery in pregnancy or postpartum
2.bone fractures operated or immobilized with prolonged gypsum
3. hyperemia, dehydration
4.ovarian hyperstimulation syndrome in assisted human reproduction process
5. prolonged hospitalization/immobilization ≥3 days
6. severe systemic infections
7. travel/long distance flights (>4 hours).
A history of venous thromboembolism associates a recurrence risk in pregnancy 20-30 times higher than the incidence of this pathology in pregnant and postpartum population(8). The incidence of venous thromboembolism in pregnant women with APS is estimated to be 5-12%. If any of the aforementioned factors are present, the pregnancy requires adapted management, by collaboration with a hematology specialist, due to the high risk for thromboembolic disease(9).
2. Indication for thrombophilic disorders screening in pregnancy
Since about 50% of venous thromboembolism in pregnancy associates hereditary or acquired thrombophilias, the screening for thrombophilic disorders should be recommended to all pregnant women who associate a history of venous thromboembolism or manifested venous thrombosis during the current pregnancy(8). Protein C and Protein S determination is less reliable during pregnancy. Protein S normally decreases by about 40% during pregnancy. A free Protein S antigen <55% in non-pregnant women should be detected at least twice to reveal Protein S deficiency. When the screening is performed during pregnancy, the second and third trimester limit values of <30% and <24%, respectively, may be valid for the diagnosis of the deficit(11).
The screening of healthy pregnant women with no previous history of venous thromboembolism, but with first-degree relatives known with hereditary thrombophilia or venous thromboembolism, is not recommended due to lack of proven benefit(11). Screening for MTHFR mutations is not recommended in the presence of a normal homocysteine status.
Following screening, the physician should categorize the case according to the identified thrombophilic mutation, depending on the degree of thromboembolic risk, in(12):
-
High risk hereditary thrombophilia
1.homozygous mutation factor Factor V Leiden (RR: 25)
2.homozygous mutation G20210A of the prothrombin gene (RR: 25)
3.compound heterozygous mutation Factor V Leiden/G20210A prothrombin (RR: 84)
4.antithrombin III activity <60% (RR: 50-100).
- Low risk hereditary thrombophilia
5.heterozygous mutation of factor V Leiden (RR: 5-7)
6.heterozygous G20210A mutation of the prothrombin gene (RR: 3-9)
7.protein C activity <50% (RR: 10-13)
8.free protein S antigen <55% (RR: 2-10).
According to the latest studies, PAI and MTHFR mutation would not alter the risk of venous thromboembolism in pregnancy, and the screening for these forms of thrombophilia is not indicated. The vast majority of patients with thrombophilia and no history of pregnancy complicated with preeclampsia, intrauterine growth restriction, stillbirth or abruption placentae have uncomplicated normal pregnancies and do not require thrombophilia tests, having a normal pregnancy outcome(11).
3. Antiphospholipid syndrome in pregnancy
The diagnosis of antiphospholipid syndrome (APS) requires the presence of at least one clinical criterion and a laboratory criterion(13).
The clinical criteria include vascular thrombosis with one or more clinical episodes of arterial, venous or small vessel thrombosis in any tissue or organ; and/or morbidity in pregnancy with:
-
one or more unexplained fetal deaths of a morphologically normal fetus at or after the 10th week and/or
-
one or more premature births of a morphologically normal newborn before the 34th week of pregnancy due to eclampsia or severe preeclampsia or features that indicate placental insufficiency (abnormal umbilical or uterine Doppler flow and/or intrauterine growth restriction <10%, oligohydramnios) and/or
-
three or more consecutive unexplained spontaneous abortions prior to the 10th week of pregnancy, in the absence of any anatomical, hormonal or chromosomal anomalies.
Laboratory criteria in APS diagnosis include lupus anticoagulant detected in plasma at two or more determinations at least 12 weeks apart (the analysis should be performed before treatment with anticoagulants) and/or IgG and/or IgM anticardiolipin antibodies detected in serum or plasma and/or anti-beta2-glycoprotein I antibodies; IgG and IgM by ELISA(14).
The screening of laboratory criteria is applied to patients who have one or more clinical criteria. It is recommended that the management of pregnancies with APS to be multidisciplinary, performed by obstetrics-gynecology, rheumatology/internal medicine and hematology specialists. APS is associated with venous thromboembolism, early onset preeclampsia, early pregnancy loss, fetal growth restriction, intrauterine fetal death, premature delivery and abruptio placentae(15).
4. The diagnosis of thromboembolic disease
A pregnant woman showing any signs or symptoms suggestive of thromboembolic disease should be urgently investigated. The first line of investigations consists of: Duplex Doppler of the lower limbs, prediction scores such as Wells, the LEFt clinical prediction rule – symptoms in the left leg (L), calf circumference difference of 2 centimeters or more (E for edema), first trimester presentation (Ft) – and D-dimers(16). A positive Duplex ultrasound confirms the diagnosis of deep vein thrombosis and anticoagulation should be started immediately(17). A negative Duplex ultrasound does not exclude deep vein thrombosis in pregnant women, and subsequent management depends on the degree of clinical suspicion. Continuing testing and empirical administration of anticoagulation are necessary in case of high clinical suspicion. If the Duplex Doppler ultrasound does not confirm the diagnosis of pulmonary thromboembolism, but symptomatology and clinical signs are present, the doctor may indicate the following investigations(18): pulmonary ventilation/perfusion scintigraphy V/Q (ventilation component may be omitted in pregnancy), CT pulmonary angiography (CTPA), magnetic resonance imaging (MRI) or contrast-based venography. The British Thoracic Society(20) recommends CTPA as the first investigation for non-massive pulmonary thromboembolism. The advantages of this technique would be greater specificity and sensitivity and lower fetal irradiation. In pregnancy, the level of D-dimers is increased due to physiological changes in the coagulation system, increasing in term and in luscious even in healthy pregnant women. Moreover, the level of D-dimers increases if there is concomitant preeclampsia(19). A low level of D-dimers suggests that there is no venous thromboembolism. In this context, a negative D-dimer assay (<500 ng/ml) has a significant negative predictive value(19).
5. Thromboprophylaxis
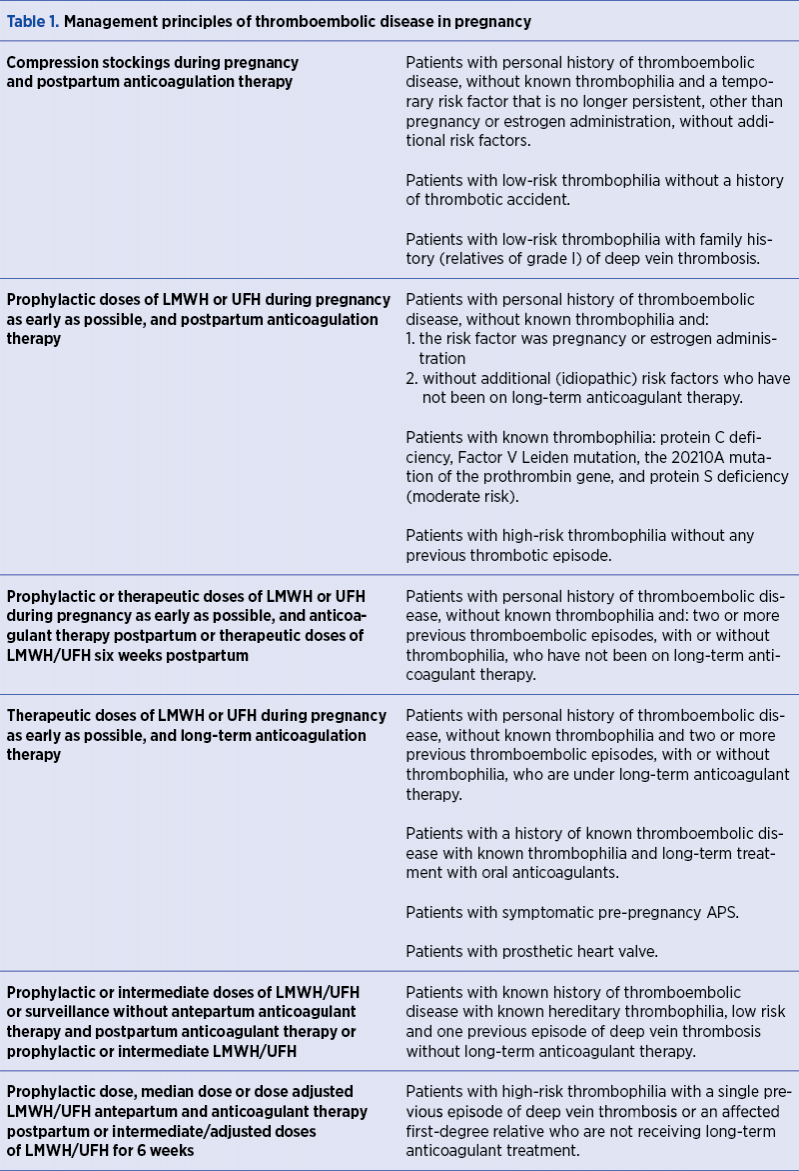
For all cases of pregnancies and postpartum women, avoidance of dehydration, an active life and, respectively, early mobilization are recommended. In Table 1 there are summarized by risk categories the main management principles of thromboembolic disease in pregnancy(20,21,22).
LMWH is the anticoagulant drug of choice, except for patients with a history of heparin-induced thrombocytopenia or with severe renal insufficiency. Alternatively, unfractionated heparin (UFH) can be used. UFH is administered either initially intravenously followed by an adjusted dose subcutaneously every 12 hours, or subcutaneously every 12 hours without the initial intravenous dose administration. UFH doses should be adjusted in order to reach an average aPTT (4-6 hours’ post-dose) within the therapeutic range(23).
For cases of pregnancies with confirmed APS, it is recommended to associate the prophylactic therapy with LMWH/UFH with low-dose aspirin as early as possible in pregnancy up to 36 weeks of gestation, since this treatment schedule has the highest efficiency in early pregnancy loss prevention with a favorable pregnancy outcome. In postpartum, the anticoagulation therapy with vitamin K antagonists may be initiated, for a INR of 3(24).
6. The treatment of venous thromboembolism in pregnancy
The anticoagulation therapy should be initiated at the moment of the venous thromboembolism diagnosis during pregnancy and continued at least six weeks postpartum. There are no significant study reports regarding the optimal duration of anticoagulation therapy in pregnancy-related venous thromboembolism, but at least three-month duration is mandatory(25). The treatment of thromboembolic disease in pregnant women and postpartum women can be performed in the obstetrics-gynecology departments, except for the cases when the in-hospital consultation (cardiologist, ATI) decides the transfer. If the diagnosis is not confirmed by ultrasound Duplex Doppler but clinical suspicion persists, the doctor may initiate anticoagulation and may indicate a repeated ultrasound at weekly intervals(25). If during these investigations the diagnosis is infirmed, the anticoagulation therapy can be interrupted.
7. The treatment of pulmonary embolism
in pregnancy
Considering the impact of pulmonary embolism in pregnancy and the required specific approach, we consider that is necessary to detail the main principles of this condition. As a rule, if there is a high clinical suspicion for acute pulmonary embolism, empiric anticoagulation therapy will be indicated immediately; in cases with low or moderate suspicion, the administration of anticoagulants is decided according to the associated condition, case-by-case(6). The useful investigations in order to confirm the suspected diagnosis are: ECG, pulmonary radiography, ventilation/perfusion scintigraphy or CT pulmonary angiogram. Subcutaneous LMWH is preferential, having a high safety and being easier to administer(7). UFH is indicated to be used if there is a high risk of bleeding, renal insufficiency or important, persistent hypotension. Considering the unknown safety of direct oral anticoagulants in pregnancy, this approach is not recommended(26). Severe cases of pulmonary embolism, life-threatening, may require thrombolysis or thrombectomy; the efficiency of these approaches in such cases exceeds the risks of maternal hemorrhage or fetal distress(27).
8. Therapeutic approach in labor of patients with anticoagulation therapy
The anticoagulation therapy should be discontinued before the onset of labor. All pregnant women should be instructed regarding the interruption of anticoagulation. If a programmed induced labor is expected, the last dose of anticoagulant should be taken 24 hours before the scheduled date of birth or caesarean section in cases of therapeutic dose therapy(28). Single daily dosed patients will only receive 50% of the usual dose in the morning of the day before birth(28). Vaginal birth is indicated when possible, caesarean surgery being a risk factor for thromboembolic disease. Neuraxial (epidural or spinal) blockage can be performed safely at over 12 hours after discontinuing prophylactic doses of anticoagulants and at over 24 hours after the discontinuation of therapeutic doses of anticoagulants. If labor occurs in a fully anticoagulated patient, neuraxial anesthesia is avoided(29). It is recommended that the doctor indicates anticoagulation at a distance of at least 6 hours after removal of the peridural catheter. The switch to UFH therapy at 36 weeks of the patients on LMWH therapy, if the onset of spontaneous labor is predicted, can be helpful considering the possibility of local anesthesia. In case of UFH therapy, regional anesthesia can usually be given between six and eight hours after dosing or at least when aPTT is within normal range(30). Birth should be considered at 39 weeks – 39 weeks and 6 days, in order to control the discontinuation time of anticoagulation(30).
Conclusions
The anticoagulant treatment should be monitored by the hematologist – obstetrician – gynecologist team, knowing that in pregnant and postpartum women receiving vitamin K antagonists, the INR should be between 2 and 3, while pregnant and postpartum women who receive unfractionated heparin should have an aPTT value between 2-3 times the laboratory reference value(26). Regarding LMWH, for women with pregnancy or puerperium receiving low-molecular-weight heparins, the doses should be adjusted to achieve an anti-factor Xa level between 0.5 and 1.2 U/ml at six hours post-administration or an anti-factor Xa level of 0.6-1 UI/ml at 24 hours post-administration(26). The anti-factor Xa level is usually generated four hours after the administration. The anti-factor Xa level is tested at least every three weeks after the initiation of heparin therapy. The initial platelet count should be verified and then weekly testing over the first three weeks is necessary to ensure that there is no evidence of heparin-induced thrombocytopenia(28). In the absence of robust data on dose adjustment during pregnancy, the following options may be considered: the initial dose remains unadjusted during pregnancy, dose adjustment according to weight change, dose adjustments based on the peak of the anti-factor Xa level to maintain its value between 0.6 and 1 u/mL(26). During the first three weeks of heparin treatment, it is indicated to monitor weekly the complete blood count and then monthly, given the heparin potential to induce thrombocytopenia, and also to advise patients to recognize the signs and symptoms of thromboembolic disease. A complete and correct management of high risk for thromboembolic disease pregnancies include multi-team collaboration, with systematic hematological evaluation of the patient. Particular aspects of fetal monitoring include serial ultrasound monitoring (4-6 weeks interval from 18-20 weeks of gestation) to assess fetal growth, and early diagnosis of potential fetal development abnormalities through amniotic fluid index monitoring, uterine artery and cerebral artery Doppler evaluation and non-stress fetal testing. An early gestation ultrasound is essential for a correct diagnosis of fetal growth restriction, frequently encountered in cases with high thromboembolic risk.
The cases of thromboembolism during pregnancy and puerperium are complex, with high mortality and morbidity risks, and require team collaboration between cardiologist, gynecologist, hematologist and intensive care specialists. The key to success for a good prognosis is the compliance with a clear, standardized, adapted protocol.
Conflict of interests: The authors declare no conflict of interests.
Bibliografie
1. Clark SL, Belfort MA, Dildy GA, et al. Maternal death in the 21st century: causes, prevention, and relationship to caesarean delivery. Am J Obstet Gynecol. 2008; 199:36.e1-36.e5.
2. Chang J, Elam-Evans LD, Berg CJ, et al. Pregnancy-related mortality surveillance – United States, 1991-1999. MMWR Surveill Summ. 2003 Feb 21; 52(2):1-8.
3. Bourjeily G, Paidas M, Khalil H, et al. Pulmonary embolism in pregnancy. Lancet. 2010; 375:500.
4.Morris JM, Algert CS, Roberts CL. Incidence and risk factors for pulmonary embolism in the postpartum period. J Thromb Haemost. 2010; 8:998.
5. Heit JA, Kobbervig CE, James AH, et al. Trends in the incidence of venous thromboembolism during pregnancy or postpartum: a 30-year population-based study. Ann Intern Med. 2005; 143:697.
6. Bates SM, Rajasekhar A, Middeldorp S, et al. American Society of Hematology 2018 guidelines for management of venous thromboembolism: venous thromboembolism in the context of pregnancy. Blood Adv. 2018; 2:3317.
7. Bates SM, Greer IA, Middeldorp S, et al. VTE, thrombophilia, antithrombotic therapy, and pregnancy: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012; 141:e691S.
8. Stein PD, Hull RD, Kayali F, et al. Venous thromboembolism in pregnancy: 21-year trends. Am J Med. 2004; 117:121.
9. American College of Obstetricians and Gynecologists. Thromboembolism in Pregnancy. ACOG 2018. ACOG Practice Bulletin. 196.
10. McColl MD, Ellison J, Reid F, et al. Prothrombin 20210 G-->A, MTHFR C677T mutations in women with venous thromboembolism associated with pregnancy. BJOG. 2000; 107:565.
11. Marik PE, Plante LA. Venous thromboembolic disease and pregnancy. N Engl J Med. 2008; 359:2025.
12. Yelnik CM, Laskin CA, Porter TF, et al. Lupus anticoagulant is the main predictor of adverse pregnancy outcomes in aPL-positive patients: validation of PROMISSE study results. Lupus Sci Med. 2016; 3:e000131.
13. Latino JO, Udry S, Aranda FM, et al. Pregnancy failure in patients with obstetric antiphospholipid syndrome with conventional treatment: the influence of a triple positive antibody profile. Lupus. 2017; 26:983.
14. Tong M, Viall CA, Chamley LW. Antiphospholipid antibodies and the placenta: a systematic review of their in vitro effects and modulation by treatment. Hum Reprod Update. 2015; 21:97.
15. Motta M, Chirico G, Rebaioli CB, et al. Anticardiolipin and anti-beta2 glycoprotein I antibodies in infants born to mothers with antiphospholipid antibody-positive autoimmune disease: a follow-up study. Am J Perinatol. 2006; 23:247.
16. Cahill AG, Stout MJ, Macones GA, Bhalla S. Diagnosing pulmonary embolism in pregnancy using computed-tomographic angiography or ventilation-perfusion. Obstet Gynecol. 2009; 114:124.
17. Revel MP, Cohen S, Sanchez O, et al. Pulmonary embolism during pregnancy: diagnosis with lung scintigraphy or CT angiography? Radiology. 2011; 258:590.
18. Chan WS, Ray JG, Murray S, et al. Suspected pulmonary embolism in pregnancy: clinical presentation, results of lung scanning, and subsequent maternal and pediatric outcomes. Arch Intern Med. 2002; 162:1170.
19. Kline JA, Williams GW, Hernandez-Nino J. D-dimer concentrations in normal pregnancy: new diagnostic thresholds are needed. Clin Chem. 2005; 51:825.
20. Bates SM, Greer IA, Middeldorp S, et al. VTE, thrombophilia, antithrombotic therapy, and pregnancy: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012; 141:e691S.
21. Roeters van Lennep JE, Meijer E, Klumper FJ, et al. Prophylaxis with low-dose low-molecular-weight heparin during pregnancy and postpartum: is it effective? J Thromb Haemost. 2011; 9:473.
22. Pettilä V, Kaaja R, Leinonen P, et al. Thromboprophylaxis with low molecular weight heparin (dalteparin) in pregnancy. Thromb Res. 1999; 96:275.
23. Bain E, Wilson A, Tooher R, et al. Prophylaxis for venous thromboembolic disease in pregnancy and the early postnatal period. Cochrane Database Syst Rev. 2014; CD001689.
24. Ziakas P, Pavlou M, Voulgarelis M. Heparin treatment in antiphospholipid syndrome with recurrent pregnancy loss. Obstet Gynecol. 2010; 115: 1256–62.
25. Goel N, Tuli A, Choudhry R. The role of aspirin versus aspirin and heparin in cases of recurrent abortions with raised anti-cardiolipin antibodies. Med Sci Monit. 2006; 12: CR132–6. [RCT, n=72]
26. van Dongen CJ, van den Belt AG, Prins MH, Lensing AW. Fixed dose subcutaneous low molecular weight heparins versus adjusted dose unfractionated heparin for venous thromboembolism. Cochrane Database Syst Rev. 2004; CD001100.
27. Ahearn GS, Hadjiliadis D, Govert JA, Tapson VF. Massive pulmonary embolism during pregnancy successfully treated with recombinant tissue plasminogen activator: a case report and review of treatment options. Arch Intern Med. 2002; 162:1221.
28. Horlocker TT, Wedel DJ, Benzon H, et al. Regional anesthesia in the anticoagulated patient: defining the risks (the second ASRA Consensus Conference on Neuraxial Anesthesia and Anticoagulation). Reg Anesth Pain Med. 2003; 28:172.
29. Wysowski DK, Talarico L, Bacsanyi J, Botstein P. Spinal and epidural hematoma and low-molecular-weight heparin. N Engl J Med. 1998; 338:1774.
30. Bates SM, Ginsberg JS. How we manage venous thromboembolism during pregnancy. Blood. 2002; 100:3470.

IN MEMORIAM DR. EMIL GHEORGHIŢĂ
Mircea Covic, Mircea Onofriescu
In November 2018, Doctor Emil Gheorghiţă died. He was a remarkable physician, a clinic and school founder, a pioneer in the medical world. Moreover, he was a very special person. Everybody loved him – colleagues, patients, relatives and friends – for his generosity, talent, culture and personal qualities....
Opinii şi recomandări curente pentru utilizarea meşei în chirurgia ginecologică – review al literaturii
L. Pirtea, Cristina Secoşan, G. Crăciun, Profira Boştină, Ligia Bălulescu, Oana Balint, Dorin Grigoras
Tratamentul prolapsului genital rămâne controversat în practica de zi cu zi, din cauza numeroaselor posibilităţi terapeutice – cu ...
Rolul 25 hidroxivitaminei D (25(OH)D) în travaliul prematur
Anak Agung Gede Putra Wiradnyana, Ketut Suwiyoga, Ketut Surya Negara
Travaliul prematur este cea mai importantă cauză de deces în cazul copiilor sub 5 ani, la nivel mondial. Etiologia travaliului prematur este adesea necunoscută. Unele concepte care încearcă să explice cauzele travaliului...
Opinii şi recomandări curente pentru utilizarea meşei în chirurgia ginecologică – review al literaturii
L. Pirtea, Cristina Secoşan, G. Crăciun, Profira Boştină, Ligia Bălulescu, Oana Balint, Dorin Grigoras
Tratamentul prolapsului genital rămâne controversat în practica de zi cu zi, din cauza numeroaselor posibilităţi terapeutice – cu ...
Rolul 25 hidroxivitaminei D (25(OH)D) în travaliul prematur
Anak Agung Gede Putra Wiradnyana, Ketut Suwiyoga, Ketut Surya Negara
Travaliul prematur este cea mai importantă cauză de deces în cazul copiilor sub 5 ani, la nivel mondial. Etiologia travaliului prematur este adesea necunoscută. Unele concepte care încearcă să explice cauzele travaliului...